
I might bore anyone who is interested, with a few points (thread) about healthcare expenditure in Ireland, but also about GP/ community-based care- all relevant with regards to #slaintecare (1/n)
This figure below shows overall expenditure per capita ($) for Ireland over the past few years (OECD 2017 data). 
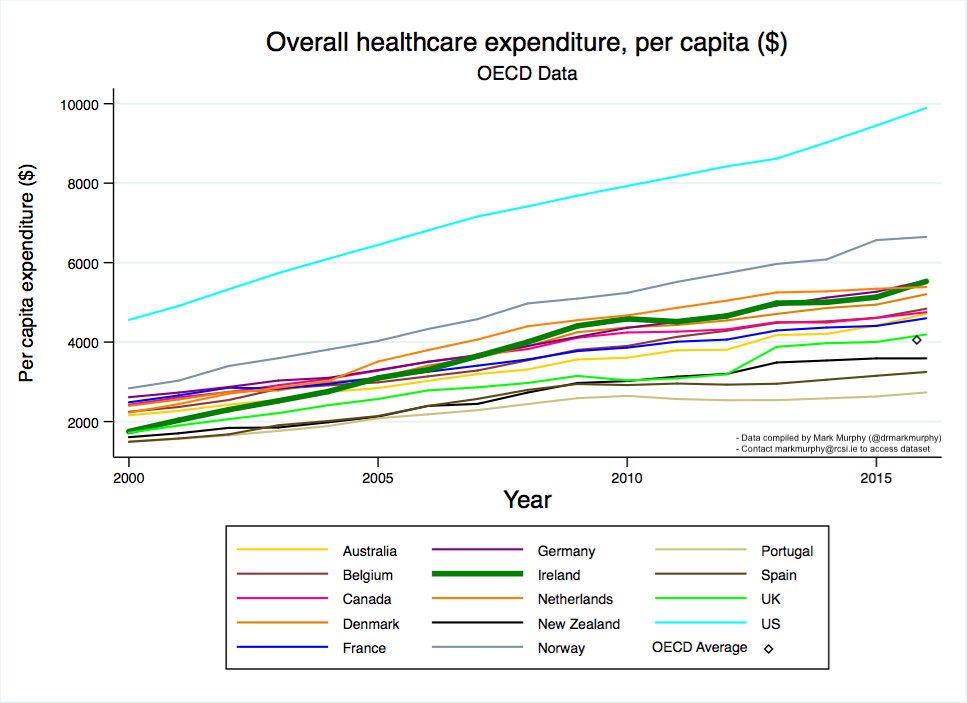
What does this tell us about overall-Irish healthcare expenditure?
So the phrase: “Ireland is one of the ‘highest spenders’ on healthcare with amongst the poorest outcomes”- a frequently heard criticism- is right?
No doubt we have high OVERALL expenditure, but we have also had:
a) A disproportionate increase in private and out of pocket expenditure over the past 4 years in particular. Ireland is 2nd from the top when it comes to private, out-of-pocket costs+voluntary insurance schemes.
a) A disproportionate increase in private and out of pocket expenditure over the past 4 years in particular. Ireland is 2nd from the top when it comes to private, out-of-pocket costs+voluntary insurance schemes.
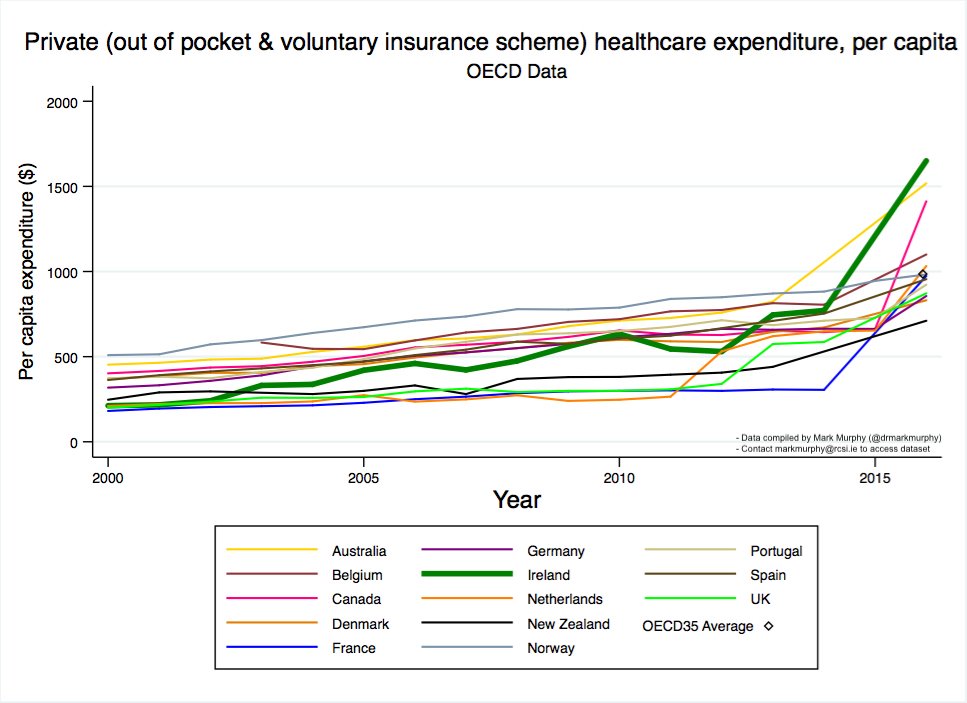
So isn’t it, mmmm, curious, that the sector of Irish healthcare that benefits from the ‘DOOMSDAY’-healthcare-narrative in Ireland… is, the private sector, which has, itself, soared. 🤔
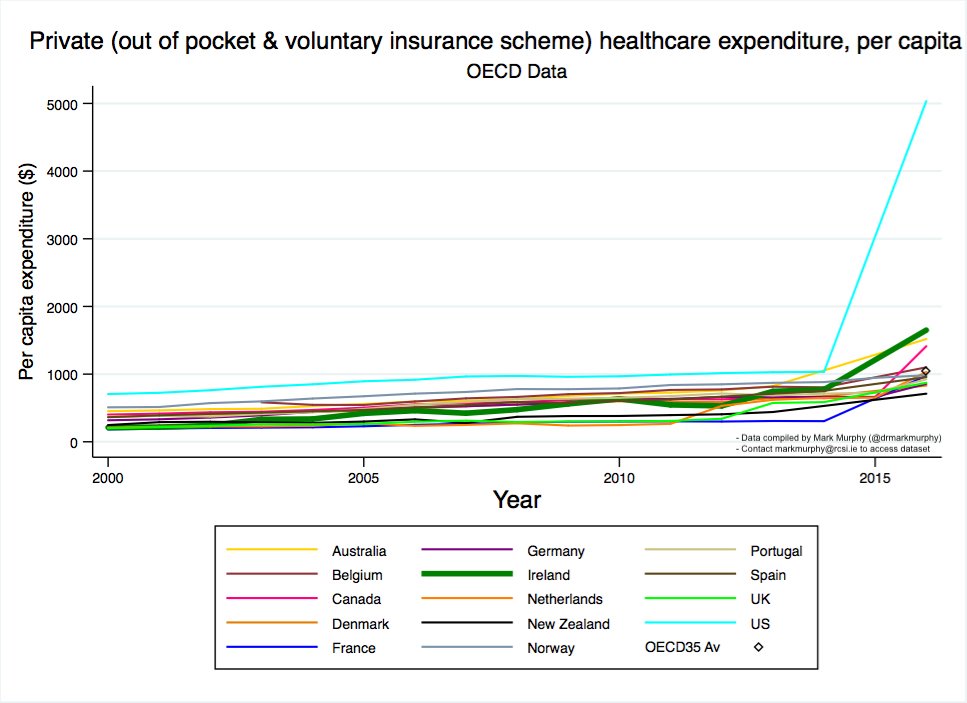
So let’s look at the second source of expenditure (again, OECD Data, 2017)
b) Government and compulsory insurance schemes.
b) Government and compulsory insurance schemes.

Yes expenditure is still very high. Yes, of course, there are governance issues, a failure to improve community-based care, problems in public healthcare…. BUT, we are not ‘the highest’ here. And we do have many favourable outcomes.

Also, as @BrianDTurner71 has articulated (see: thelancet.com/journals/lance…) we have a lot of ground to make up- compensating for erstwhile under-spending. @stephenkinsella has also pointed out our low capital spend for decades.
So we are spending more and more. Here’s the interesting thing. What exactly is the increase in expenditure actually going on?!!!
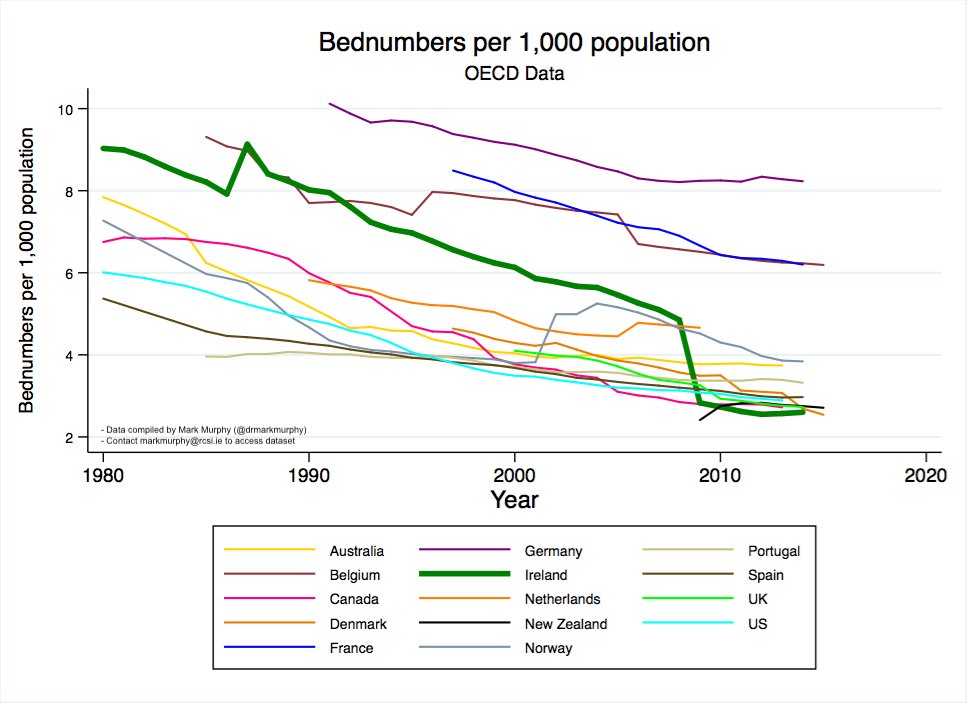
Let’s look at hospital beds firstly (courtesy of 2017 OECD data).
Yes, that cliff of a green-line is right. From the top - to the bottom… What was going on??!!
(Read the Irish Sweep if interested in a history of why we are SO hospital centric and SO non-community centric)
Yes, that cliff of a green-line is right. From the top - to the bottom… What was going on??!!
(Read the Irish Sweep if interested in a history of why we are SO hospital centric and SO non-community centric)

Just to confirm… That last graph is right!….. The 2000-governments and Drumm in the HSE did that to the system- gutting our hospitals of acute beds. Surely they had a concurrent plan, as this policy unfolded.
Was it?
Was it?
Well one would assume they would have pushed for more community-based care…. There was this 2001 strategy after all (health.gov.ie/blog/publicati…).
Let’s see what the OECD and Irish data says....
Let’s see what the OECD and Irish data says....

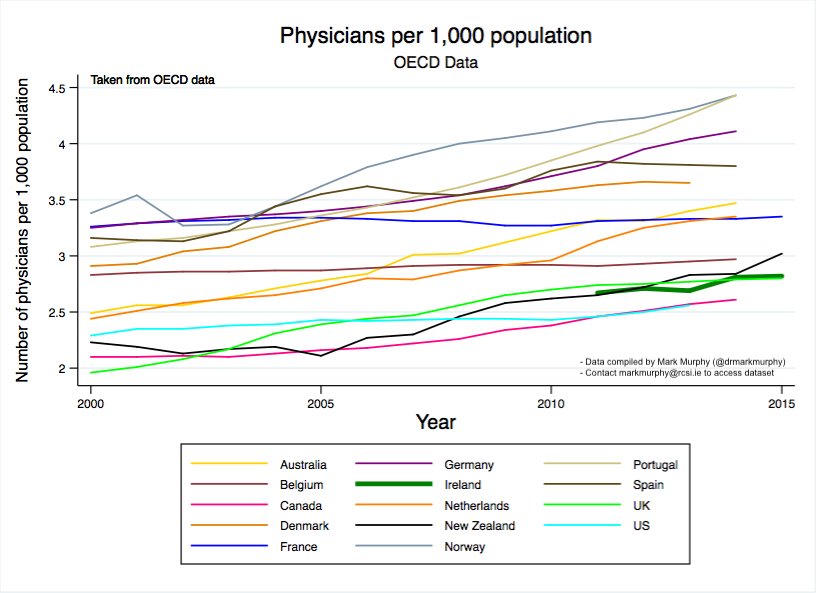
How are we doing with GP numbers? (OECD Data 2017)
(HINT- second behind the States is generally not a good thing in health system analysis).
(HINT- second behind the States is generally not a good thing in health system analysis).

But we opened up ‘the market’ to enable young GPs set up- let’s look at the PCRS Data. The number of GMS GP contracts has risen since 2000, but not recently.... Guess that famous 'market' in healthcare is not working.

Okay so we are not succeeding with training and recruiting more GPs, but we are spending more and more on health- so if we are spending so much more, surely more funding is going into General Practice (PCRS Data)


What do these last graphs show?
a) We only spend ~ >3% of the (overall) health budget on General Practice- and it has not risen. In most countries government spends > 7-8% of the overall-expenditure on care in General Practice.
a) We only spend ~ >3% of the (overall) health budget on General Practice- and it has not risen. In most countries government spends > 7-8% of the overall-expenditure on care in General Practice.
b) The blue line shows a drop in the cost per patient for GMS-GP care.
This ladies & gentlemen is #FEMPI-taking money out of providing care for patients in GP, at a time when overall expenditure is increasing in healthcare and we should be moving towards community care.
This ladies & gentlemen is #FEMPI-taking money out of providing care for patients in GP, at a time when overall expenditure is increasing in healthcare and we should be moving towards community care.
So now… let’s think about free-GP-care.
Suffice to say it is politically charged (COI- I support universal GP care, * if resourced * [this isn’t actually a COI]).
How many persons currently have free GP care? (PCRS Annual Report data).
Suffice to say it is politically charged (COI- I support universal GP care, * if resourced * [this isn’t actually a COI]).
How many persons currently have free GP care? (PCRS Annual Report data).

With GP eligibility, it is very important to reflect on the fact that:
a) Medical cards are expensive (free GP care, free medicines, free primary care etc.)
b) Doctor visit cards are cheaper for the government (only free GP care).
a) Medical cards are expensive (free GP care, free medicines, free primary care etc.)
b) Doctor visit cards are cheaper for the government (only free GP care).
As you can see there has been a shift- an overall drop- in medical cards and a huge increase in DVCs (explained by U6 and O70s). In a weird way this gives more and more persons, less care (but saves the health system €).
So now we have just less than 50% of the population having an entitlement to free GP care (granted for acute care only with a 40 year old contract with a few bandages).
** IF NOTHING CHANGES *** can we realistically enable more persons to see their GP ‘for free’- increasing eligibility with DVCs- in the coming few years?
But, I’m optimistic. *Let’s change*. Currently, in the State, GPs see the ‘heaviest-users’ in the health system already. The 45% of the population with free care are the poorest and most vulnerable/ marginalised, the Under-6s, and the Over-70s. They consult frequently.
It also may be my political belief (nothing wrong with that) that it is wrong that persons have to pay the full cost to see a GP. In time, I definitely think we can get more of the population on board. BUT…. not in next 2-3 years (if only we had a 10 year plan….)
Might also be nice if GPs had a contract that was not FOUR DECADES OLD- before modern medicine was invented. And access to diagnostics. And we fixed ICT, personnel and infrastructural capacity in existing practices (and didn’t focus on white elephant PCC buildings).
So what exactly is gobbling up the community budget in healthcare in the interim?
(HINT THIS DOESN’T HELP)
(HINT THIS DOESN’T HELP)


As @jamesfomahony said, it is the healthcare equivalent to flat-earthism, to deny ‘opportunity cost’. What would you choose, as an alternative to the provision of a VERY expensive drug (with limited benefit)?
Alas, we will need more community-based resources, in general, and this is a political decision to not enable same.
Before this thread ends, I might reflect back on some important graphs.
Bed Numbers gutted.
Concurrent to a:
Plateau in GP numbers +
Reduction in GP income
=
WHAT THE HELL DID WE EXPECT WOULD HAPPEN?
Bed Numbers gutted.
Concurrent to a:
Plateau in GP numbers +
Reduction in GP income
=
WHAT THE HELL DID WE EXPECT WOULD HAPPEN?



And ultimately, this goes back to the first slide:
“Ireland has one of the most expensive healthcare systems in the world”.
End result, yet more private-expenditure, which increases overall-spending further (in the wrong places).
🙄
“Ireland has one of the most expensive healthcare systems in the world”.
End result, yet more private-expenditure, which increases overall-spending further (in the wrong places).
🙄
Final tweet (honestly).
There is a solution.
It is called #slaintecare. Cross-party support. Fix our hospitals. Fix our community healthcare. Fix the governance. Significant investment will be needed- and has been acknowledged. #letsdothis
There is a solution.
It is called #slaintecare. Cross-party support. Fix our hospitals. Fix our community healthcare. Fix the governance. Significant investment will be needed- and has been acknowledged. #letsdothis
• • •
Missing some Tweet in this thread? You can try to
force a refresh



