What is hepatorenal syndrome?
A #Livertwitter #tweetorial
Hepatology is awesome, exciting, but also humbling.
Nowhere is that clearer than HRS, a true unmet need for patients with ascites
Aims
1. What
2. Why
3. How to prevent/treat
4. ❤️ #cirrhosis physiology
A #Livertwitter #tweetorial
Hepatology is awesome, exciting, but also humbling.
Nowhere is that clearer than HRS, a true unmet need for patients with ascites
Aims
1. What
2. Why
3. How to prevent/treat
4. ❤️ #cirrhosis physiology
What:
1. Ascites trashes QOL & is deadly enough to merit mention in the bible(Fig1)
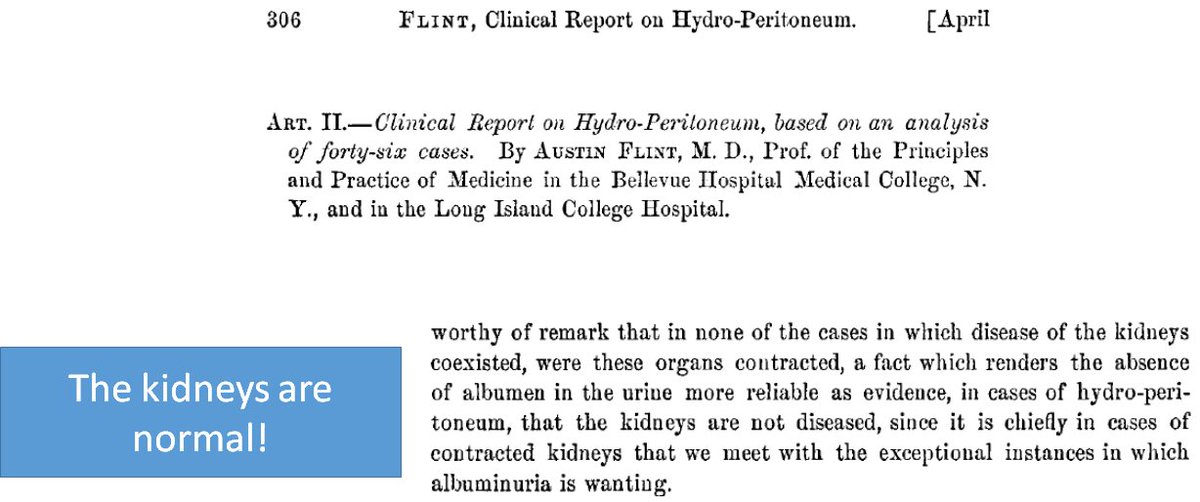
2. Ascites physiology damages other organs; Austin Flint said it 1st (Fig2)
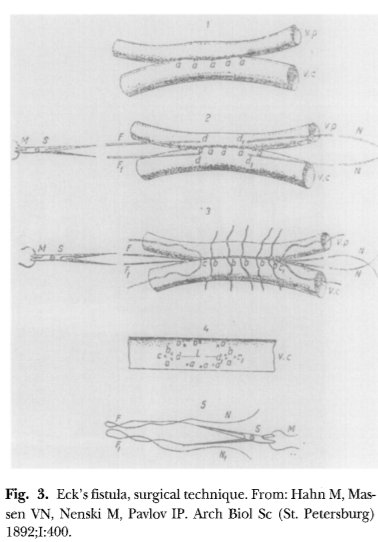
3. HRS is the knockout punch of portal hypertension. What begins as elevated portal mmHg and ascites ends as HRS(Fig3)
1. Ascites trashes QOL & is deadly enough to merit mention in the bible(Fig1)
2. Ascites physiology damages other organs; Austin Flint said it 1st (Fig2)
3. HRS is the knockout punch of portal hypertension. What begins as elevated portal mmHg and ascites ends as HRS(Fig3)



What:
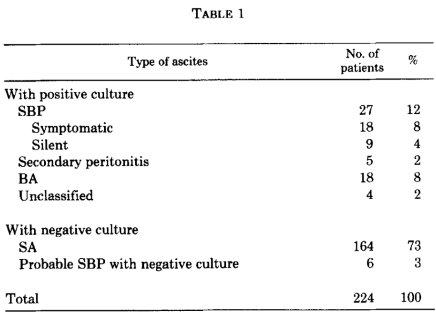
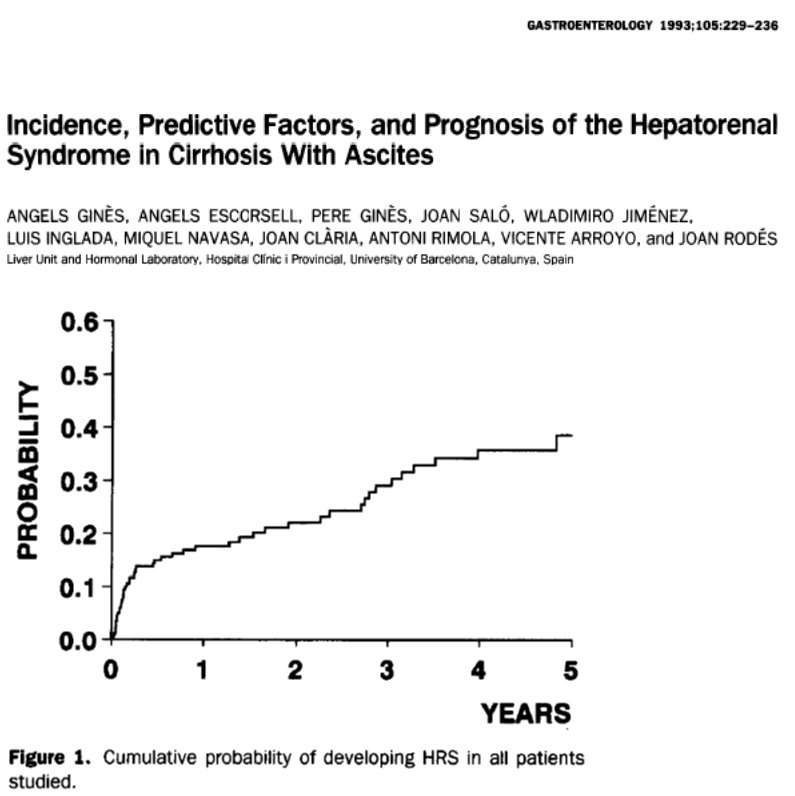
1. HRS is not rare in pts w/ascites (Fig1)
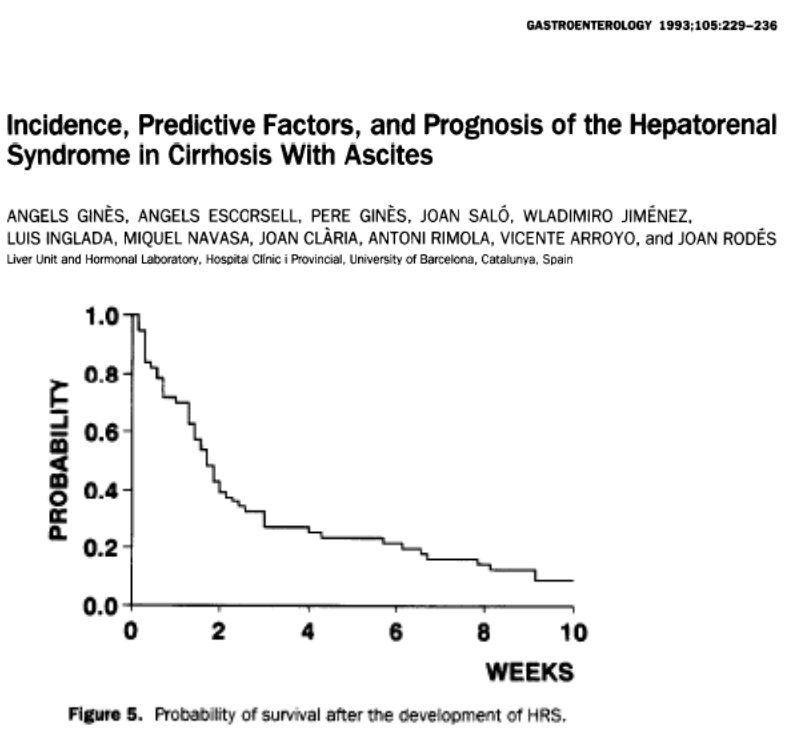
2. HRS is deadly (Fig2)
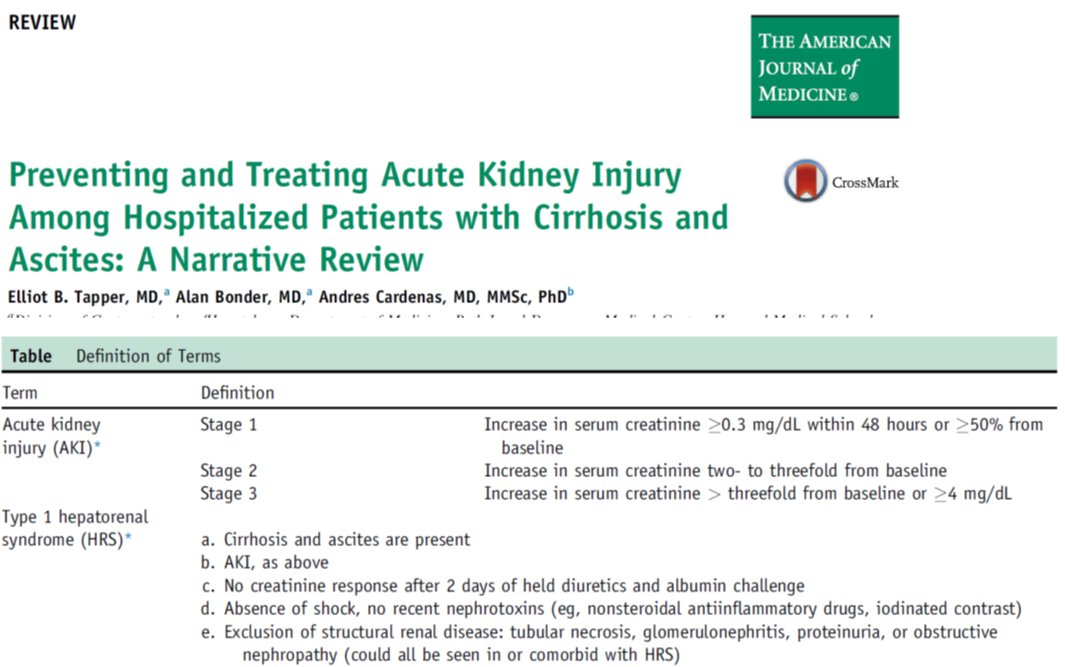
3. For a definition of terms, check out the Ascites Club (that's a thing!)
ref: gut.bmj.com/content/gutjnl…
or see my review: amjmed.com/article/S0002-… (Fig3)
1. HRS is not rare in pts w/ascites (Fig1)
2. HRS is deadly (Fig2)
3. For a definition of terms, check out the Ascites Club (that's a thing!)
ref: gut.bmj.com/content/gutjnl…
or see my review: amjmed.com/article/S0002-… (Fig3)
This is where HRS gets wild
1. The kidneys are (mostly) normal(Fig1)
2. Take the kidneys of someone who died from HRS, transplant them into someone without cirrhosis and they work just fine (Fig2)
3. Replace the liver of someone with HRS & the kidneys may wake back up(Fig3)
1. The kidneys are (mostly) normal(Fig1)
2. Take the kidneys of someone who died from HRS, transplant them into someone without cirrhosis and they work just fine (Fig2)
3. Replace the liver of someone with HRS & the kidneys may wake back up(Fig3)


What's going on in HRS?
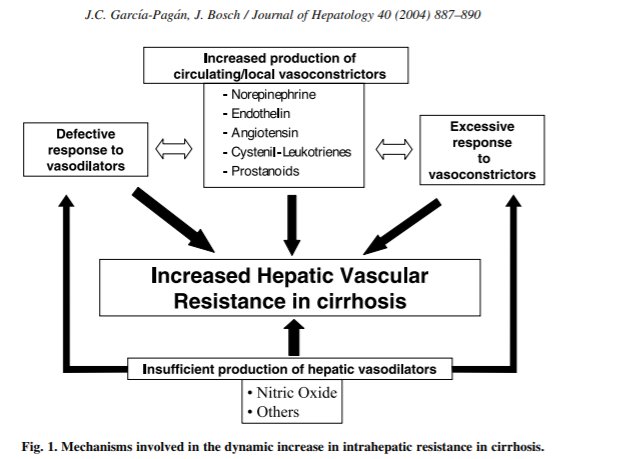
1. #Cirrhosis is a traffic jam 4 portal inflow (Fig 1)
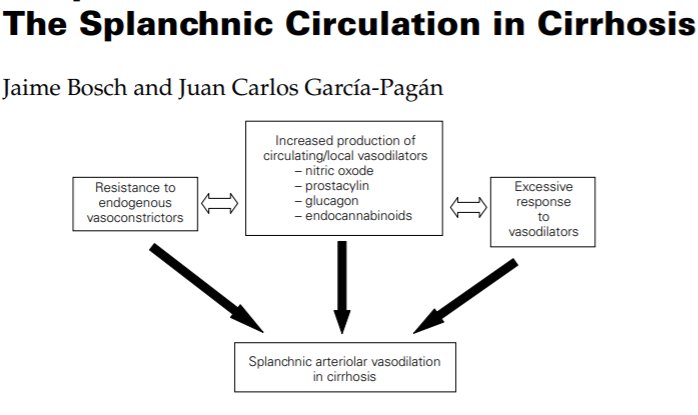
2. Splanchnic (gut) vascular bed vasodilates 🔼 pooling of blood (Fig2)
3. This means🔽return to the ❤️
4. Carotid baroreceptors, ADH, and RAAS to the "rescue" (Fig3)
1. #Cirrhosis is a traffic jam 4 portal inflow (Fig 1)
2. Splanchnic (gut) vascular bed vasodilates 🔼 pooling of blood (Fig2)
3. This means🔽return to the ❤️
4. Carotid baroreceptors, ADH, and RAAS to the "rescue" (Fig3)
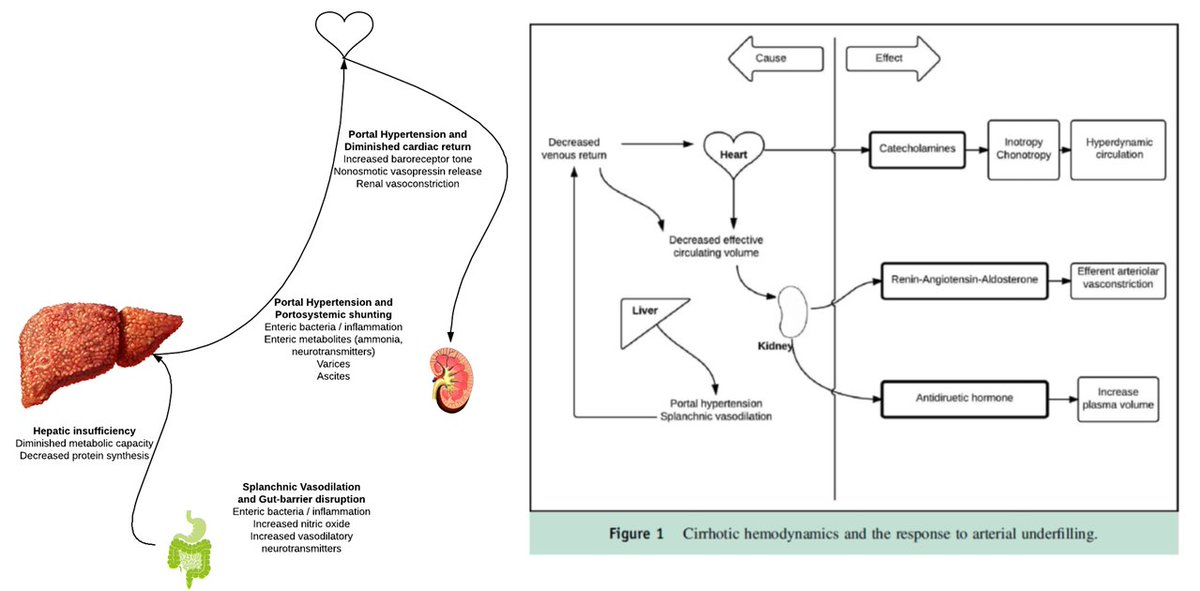
HRS is: compensatory mechanisms gone awry
To maintain ❤️ output:
Baroreceptors ▶️catecholamines, ADH
The kidney 🔼🔼 RAAS
The result?
1. Hyperdynamic circ (F1) (or just look @ a TTE)
2. Salt avidity (F3)
3. 🔼Circulatory volume (F2)
but this results in a very tenuous situation
To maintain ❤️ output:
Baroreceptors ▶️catecholamines, ADH
The kidney 🔼🔼 RAAS
The result?
1. Hyperdynamic circ (F1) (or just look @ a TTE)
2. Salt avidity (F3)
3. 🔼Circulatory volume (F2)
but this results in a very tenuous situation



HRS: All about glomerular perfusion pressure
1. Cirrhosis🔽arterial BP, RAAS/catecholes squeezw the efferent arteriole 2 maintain renal perfusion(Fig1)
2. To keep the afferent open, need prostaglandins(Fig2)
3. If thromboxane>PG🔽renal blood flow(Fig3)
Then comes calamity(Fig4)
1. Cirrhosis🔽arterial BP, RAAS/catecholes squeezw the efferent arteriole 2 maintain renal perfusion(Fig1)
2. To keep the afferent open, need prostaglandins(Fig2)
3. If thromboxane>PG🔽renal blood flow(Fig3)
Then comes calamity(Fig4)




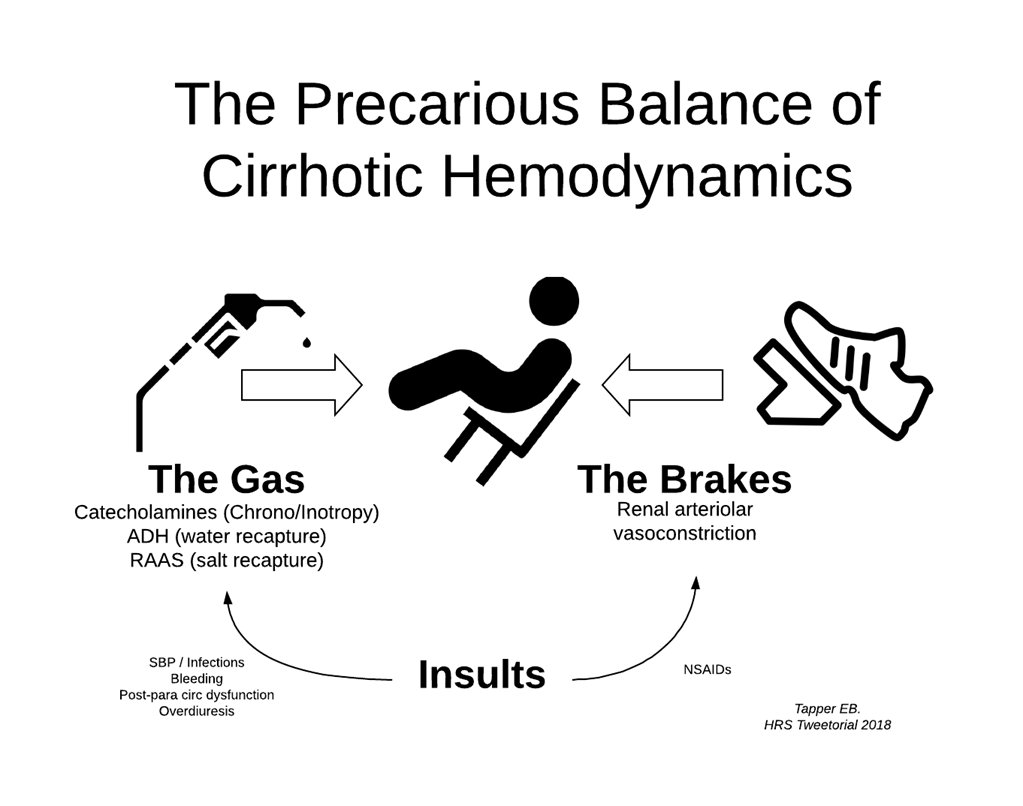
Precarious cirrhotic hemodynamics: Like driving w/one🦶on the gas, one on the breaks
(CO=HR*SV)
1. The gas pedal: Splanch pooling 🔽SV; ❤️🔼HR & contractility
2. The tank: To🔼SV we🔼ADH,Aldo
3. The breaks: RAAS/catechole r good, till they aint
Empty tank▶️all breaks▶️HRS
(CO=HR*SV)
1. The gas pedal: Splanch pooling 🔽SV; ❤️🔼HR & contractility
2. The tank: To🔼SV we🔼ADH,Aldo
3. The breaks: RAAS/catechole r good, till they aint
Empty tank▶️all breaks▶️HRS

What can you do to prevent HRS?
1. If severe infection (e.g.SBP)🔼vasodilation▶️empty tank: Give albumin!(Fig1)
2. If lrg volume para▶️6-8g/L removed albumin!
3. NO NSAIDS in patients w/ascites!!!(Fig3)
4. Don't miss SBP, temporarily hold anti-HTN meds if at risk for HRS(Fig3)
1. If severe infection (e.g.SBP)🔼vasodilation▶️empty tank: Give albumin!(Fig1)
2. If lrg volume para▶️6-8g/L removed albumin!
3. NO NSAIDS in patients w/ascites!!!(Fig3)
4. Don't miss SBP, temporarily hold anti-HTN meds if at risk for HRS(Fig3)



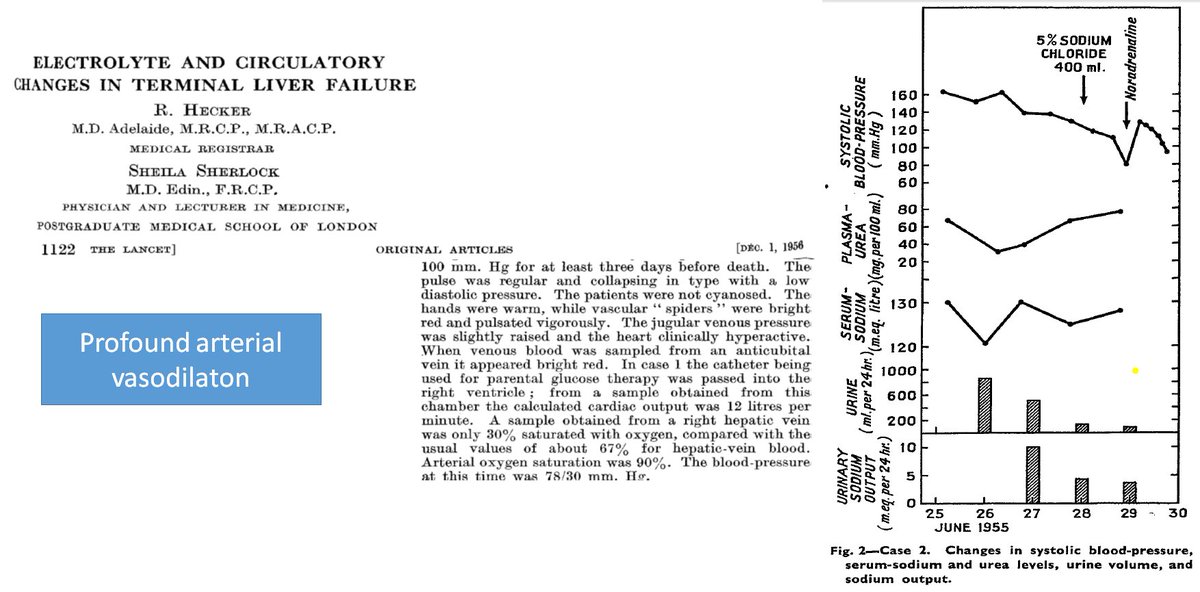
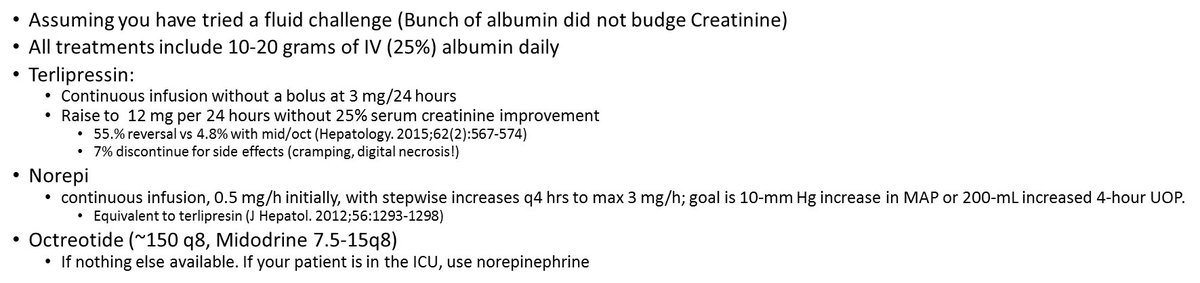
How to treat HRS?
1. Like most things in #hepatology, Sheila Sherlock did it first. (obit: aasldpubs.onlinelibrary.wiley.com/doi/abs/10.105…)
2. In 1956, she was first to note arterial vasodilation and first to use Norepi to treat HRS (Fig2)
3. Today: Albumin + Terli>/=Norepi>Midodrine/Octreo
1. Like most things in #hepatology, Sheila Sherlock did it first. (obit: aasldpubs.onlinelibrary.wiley.com/doi/abs/10.105…)
2. In 1956, she was first to note arterial vasodilation and first to use Norepi to treat HRS (Fig2)
3. Today: Albumin + Terli>/=Norepi>Midodrine/Octreo

This concludes a HRS #tweetorial.
The #cirrhosis #QI takeaways
1. Dont miss SBP (early dx para when admitted)
2. 🚫NSAIDs if ascites
3. Albumin w/therapeutic paras
Please @ me if u have anything to add!
If U want more #cirrhosis physiology, the refs are embedded in the figs
The #cirrhosis #QI takeaways
1. Dont miss SBP (early dx para when admitted)
2. 🚫NSAIDs if ascites
3. Albumin w/therapeutic paras
Please @ me if u have anything to add!
If U want more #cirrhosis physiology, the refs are embedded in the figs
See below for this post without spelling errors
Precarious cirrhotic hemodynamics: Like driving w/one🦶on the gas, one on the brakes
(CO=HR*SV)
1. The gas pedal: Splanch pooling 🔽SV; ❤️🔼HR & contractility
2. The tank: To🔼SV we🔼ADH,Aldo
3. The brakes: RAAS/catechole r good, till they aint
Empty tank▶️all brakes▶️HRS
(CO=HR*SV)
1. The gas pedal: Splanch pooling 🔽SV; ❤️🔼HR & contractility
2. The tank: To🔼SV we🔼ADH,Aldo
3. The brakes: RAAS/catechole r good, till they aint
Empty tank▶️all brakes▶️HRS
• • •
Missing some Tweet in this thread? You can try to
force a refresh