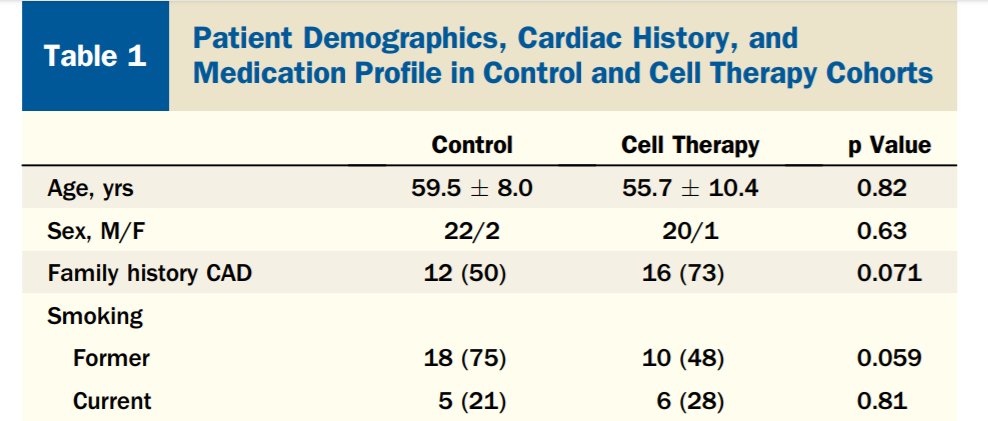
Considering #statin in 35-y-o man worried about extensive family history of MI+stroke: 2 parents, 3 of 4 sibs.
#Cholesterol 5.8 mM, 224 mg/dl. Subtypes typical for such a total.
Non-smoker. Otherwise average.
[Live-quiz from #orbita-HQ for #cardioTwitter fellows & the curious]
#Cholesterol 5.8 mM, 224 mg/dl. Subtypes typical for such a total.
Non-smoker. Otherwise average.
[Live-quiz from #orbita-HQ for #cardioTwitter fellows & the curious]
Question C2.
First vote was for diet first, and quite right too! That is the guideline, and we must obey.
Natural, organic, eco-friendly and therefore best.
What effect size is a reasonable expectation, for patient and Dr, for the reduction of total cholesterol by diet?
First vote was for diet first, and quite right too! That is the guideline, and we must obey.
Natural, organic, eco-friendly and therefore best.
What effect size is a reasonable expectation, for patient and Dr, for the reduction of total cholesterol by diet?
• • •
Missing some Tweet in this thread? You can try to
force a refresh