Artifacts in a nutshell 👽👾
A Tweetorial...
Dedicated to @bcostelloMD, @RezaEmaminia & all the great #FITs stressed out by #EchoBoards @ASE360 #carrotsquad
Images and some of the content from Bertrand, et al. JASE 2016;29:381-91. onlinejase.com/article/S0894-…
A Tweetorial...
Dedicated to @bcostelloMD, @RezaEmaminia & all the great #FITs stressed out by #EchoBoards @ASE360 #carrotsquad
Images and some of the content from Bertrand, et al. JASE 2016;29:381-91. onlinejase.com/article/S0894-…
Ultrasound waves need a media to travel. Our tissues are that media. All tissues have different acoustic impedances. Air, fat, water, blood, muscle, bone listed in increasing impedance. Always there will be reflected & refracted waves as it traverses different tissue layers. 

Remember that the way the US distributes the waves in a phased array probe is similar to a folding fan, so reflection (rebound) & refraction (change in direction) occurs across the sector width (Triangle area where you see the images) look at panel B of above figure.
The gel decreases the impedance of the skin, so the US waves can travel back & forth adequately.
Reverberation=strong reflector (calcified stuff, scar, collagenous structure, pericardium, etc) reflects some US waves back to the probe material, and rebounds again. This is registered as posterior echogenicity(-ies). Distance ratio is preserved.

Mirror artifact is a super “reverberation” a large strong reflector, typically the pericardium, causes duplication of a large structure of the heart & typically the artifact (👽) would be posterior to that large reflector. Expect to see mirror images.
Refraction= are you seeing double?? There will be a tissue that can behave as a lens & redirect part of the waves as a double image. it can obscure the structures of interest. Change the imaging plane to avoid the “lens”. Don’t confuse with mirroring

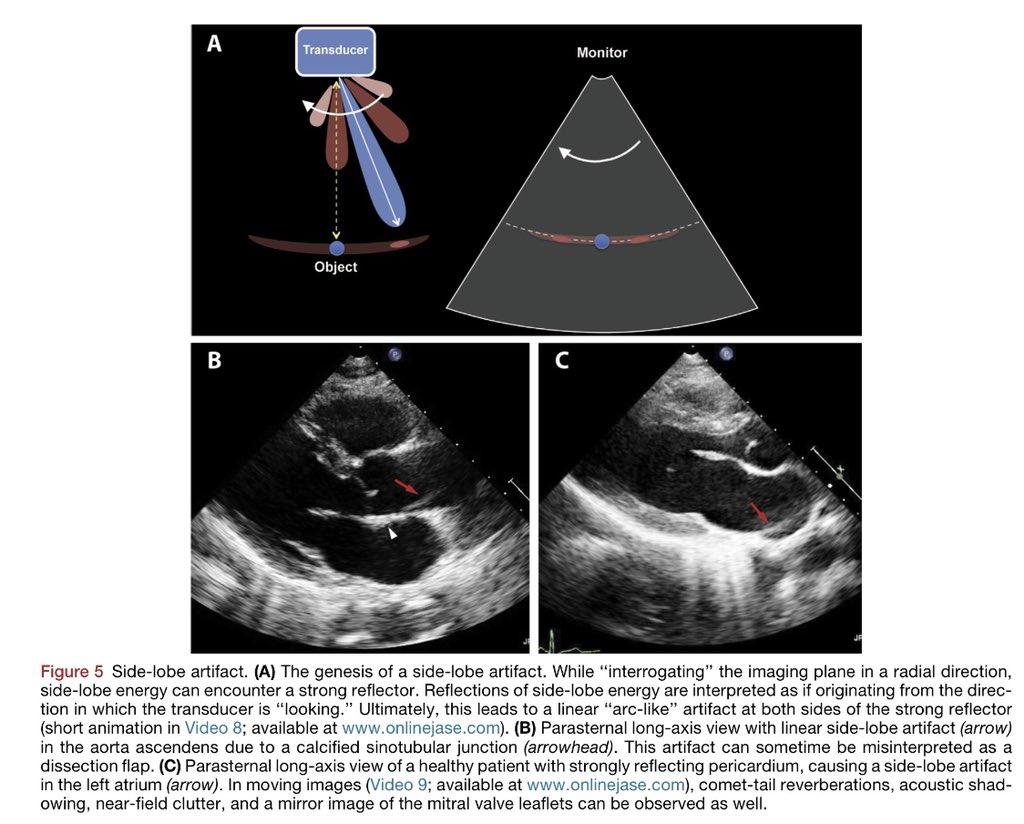
Side lobe. Nope, not all artifacts are side lobes!!! Look for a linear “arc-like” structure.Careful to confuse it with dissection or thrombus.Because it occurs when moving probe in radial direction, one of the key findings is that the artifact will traverse chambers & structures
Another that sounds complicated, but is easy. Beam width is just that, limited plane of interrogation. The elevation component of the beam might register flows or structures out of plane. You just need to change your plane to explain from where the 👽 is coming from.

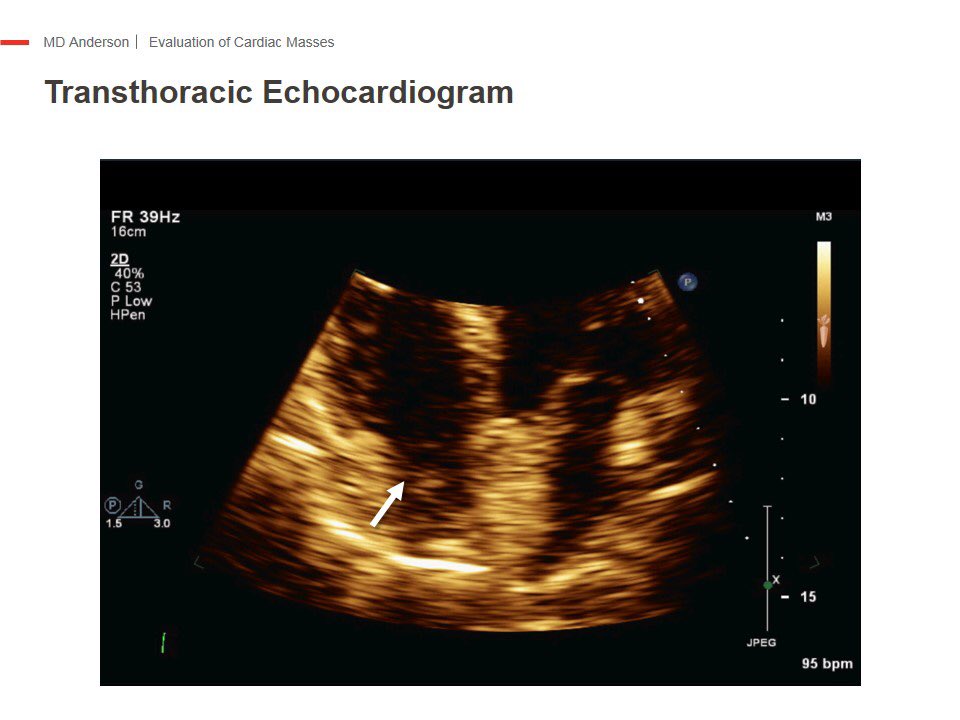
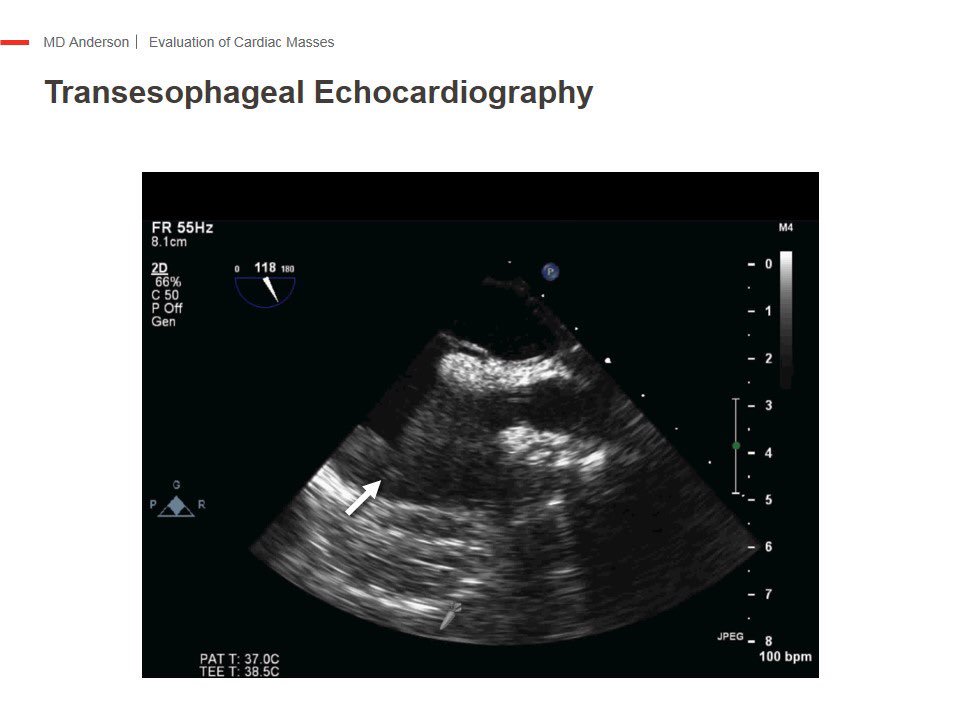
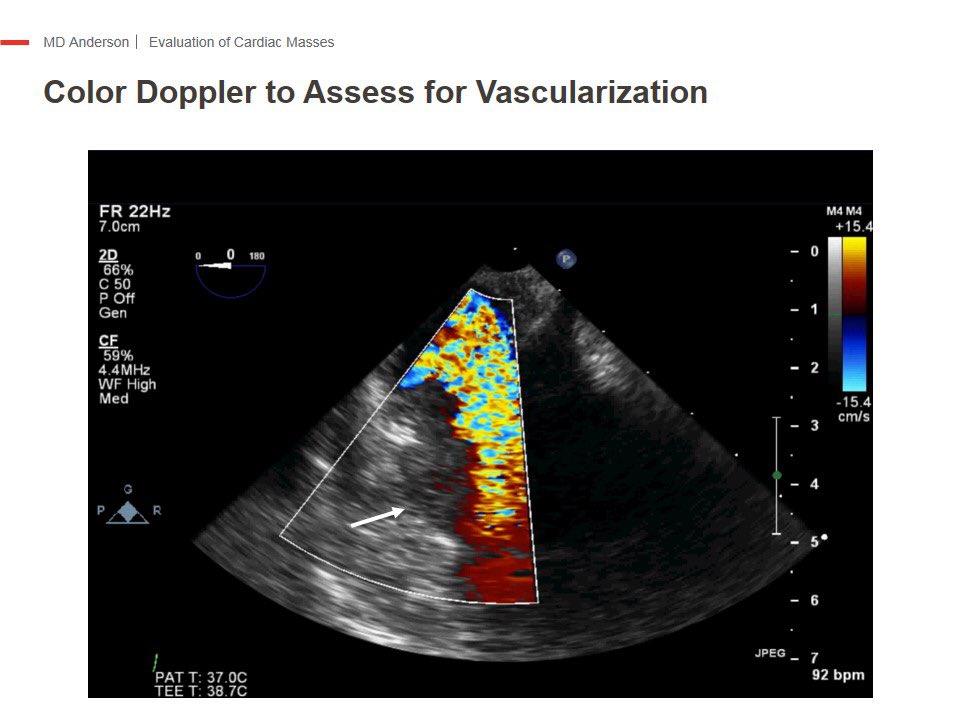
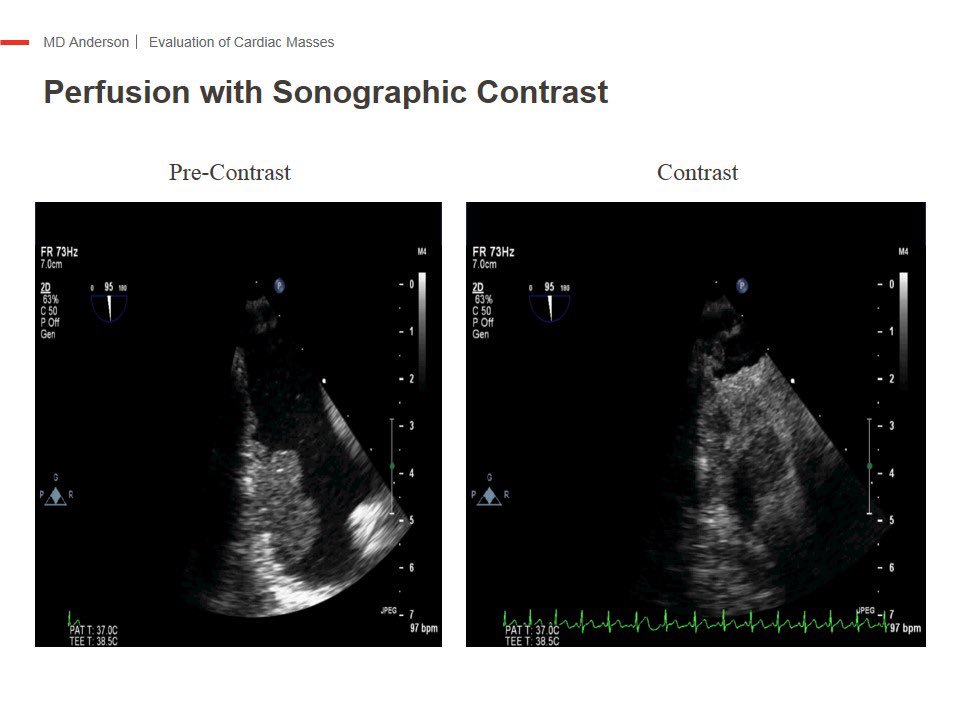
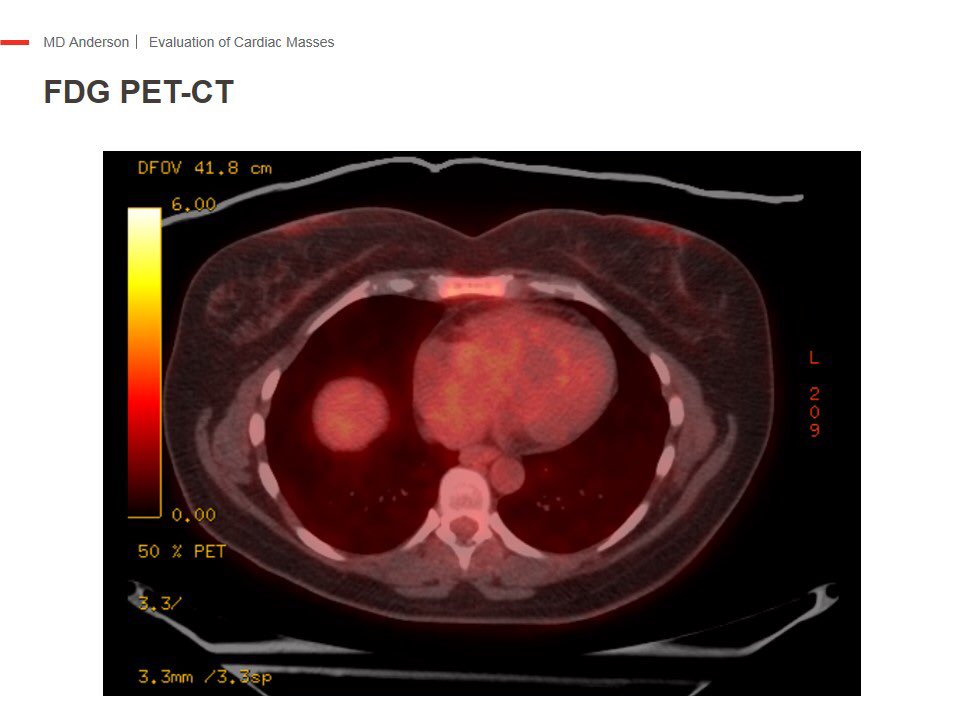
Near field clutter is classically the “pseudo thrombus” in an well contracting apex. Can give you a headache in pts with low LVEF or akinetic apex. High frequency oscillations in the “Fresnel” very close to transducer are guilty of that. If in doubt, color Doppler or contrast.

Expect multiple artifacts from prosthetic devices. Sometimes combination of TTE & TEE assessments are necessary to sort things out. They have high acoustic impedances as you would expect. Nice examples below. The amplatzer devices 👽 can be kaleidoscopic.😆

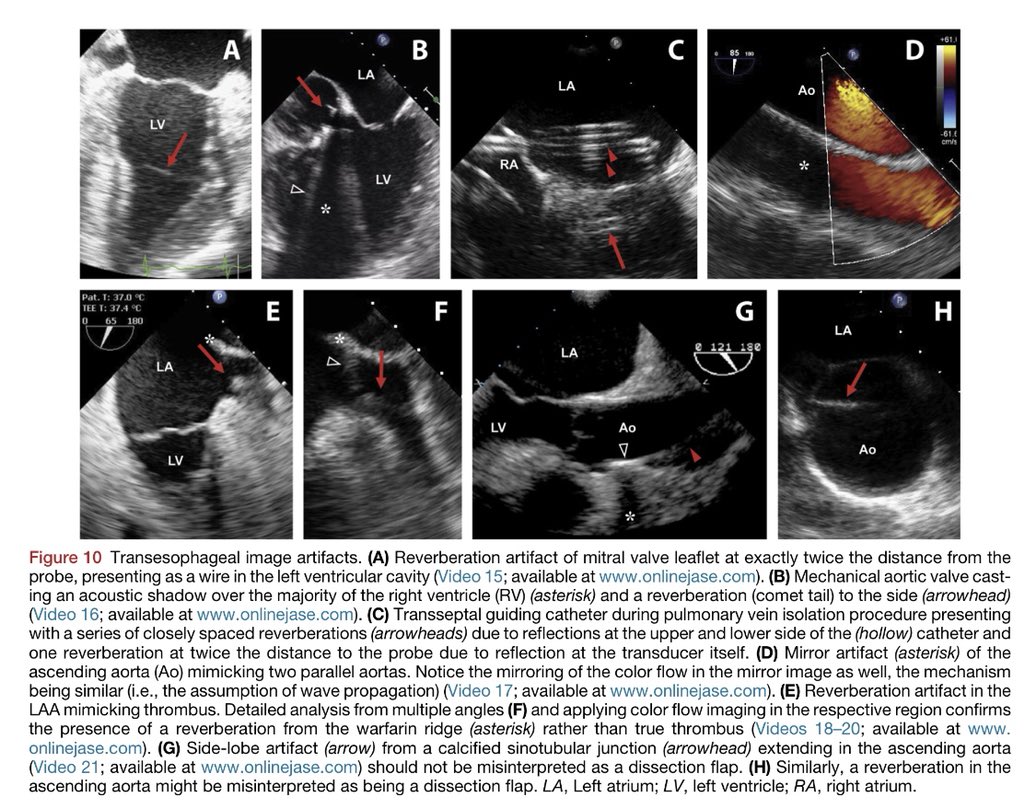
TEE artifacts can be quite scary, but after omniplaning it’s relieving to see that they are 👽. In the aorta if you see a linear structure, see if you see that line outside the aorta, use color Doppler to see if there is turbulence or difference in color Doppler in flows.
A lot of this artifacts (👽) can be improved with lowering the gain. Below tables are very useful for your boards.


@HeartOTXHeartMD @mswami001 @HeartToProve @ChamsiPash @venkmurthy @RogueRad @iamritu @cshenoy3 @SamRRazaMD @AChoiHeart @DrMarthaGulati @mariovar55 @purviparwani @almasthela @DrRyanPDaly @strain_rate @JoaoLCavalcante
• • •
Missing some Tweet in this thread? You can try to
force a refresh