Discover and read the best of Twitter Threads about #ACCFIT
Most recents (13)

1/ A long thread on LifeVest. I promise it will be entertaining. If you find any inaccuracies please let me know.
Paper of VEST published here - will discuss background to WCD and #VEST but not the trial itself nejm.org/doi/full/10.10…
Paper of VEST published here - will discuss background to WCD and #VEST but not the trial itself nejm.org/doi/full/10.10…
2/ In 2001, FDA gave approval to Lifecor for the first WCD. Later Lifecor was acquired by Zoll (2004 agreement, 2006 acquisition). Zoll maintains a registry for prescribed LifeVests. But lets go back to the FDA approval process.
3/ Lifecor presented 2 separate prospective studies to the FDA; WEARIT and BIROAD. FDA asked for both to be combined into 1 study, and each study representing a subgroup. A total of 289 patients were included.

Evaluation of Cardiac Masses:
A Tweetorial for #FITSurvivalGuide 🚨 #ACCImaging @ASE360 @SCMR @journalofCMR @ACCinTouch
Dedicated:@dr_chirumamilla & all #ACCFIT in #CardioTwitter
Main Ref: link.springer.com/article/10.100… Palaskas, et al. Curr Treat Options Cardio Med (2018) 20: 29.
A Tweetorial for #FITSurvivalGuide 🚨 #ACCImaging @ASE360 @SCMR @journalofCMR @ACCinTouch
Dedicated:@dr_chirumamilla & all #ACCFIT in #CardioTwitter
Main Ref: link.springer.com/article/10.100… Palaskas, et al. Curr Treat Options Cardio Med (2018) 20: 29.

Usually, it all starts with an abnormal finding in an echo suggestive of intracavitary mass. How can we tell one from the other? It can be confusing.

For artifacts, I did a Tweetorial already that describes the most common ones. Basic understanding of ultrasound physics is needed to be able to explain them: twitter.com/i/moments/1030…

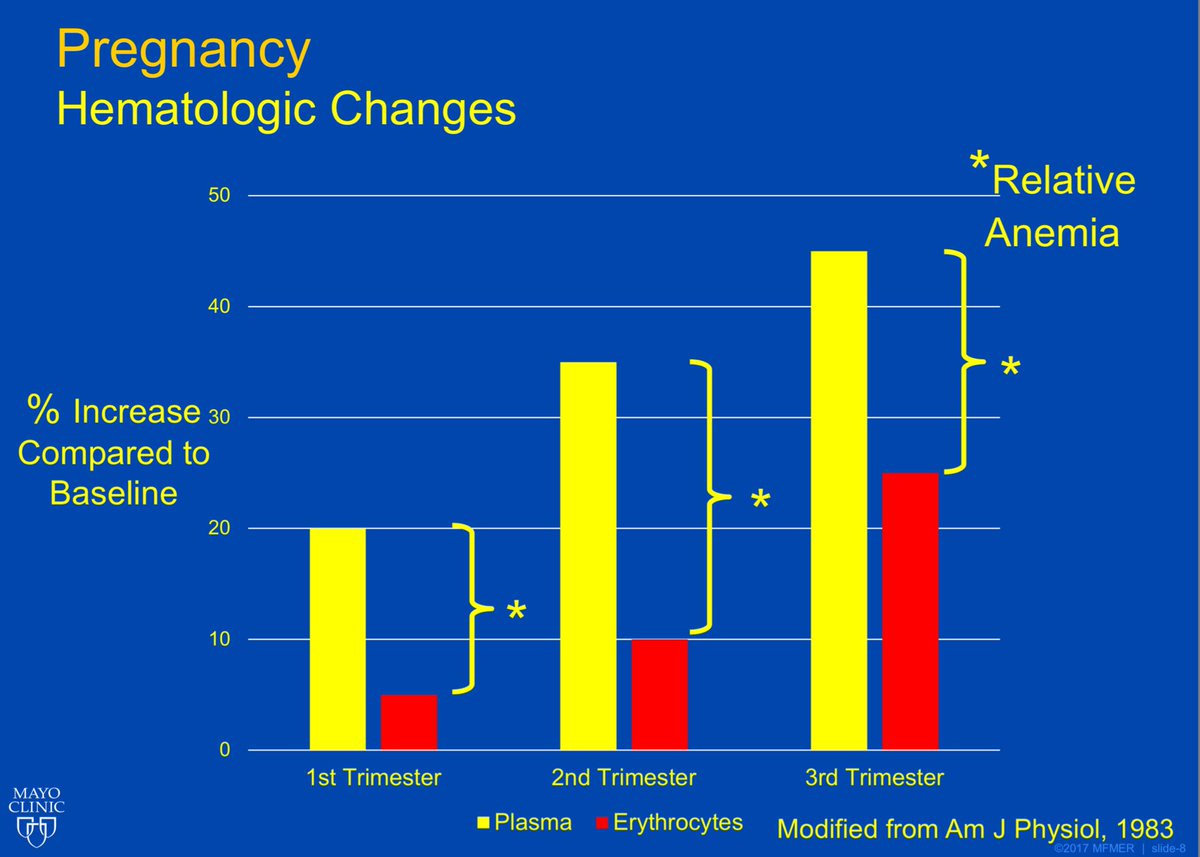
#PregnancyCardiology Primer courtesy of a fantastic lecture by Dr. Sabrina Phillips from Mayo Clinic. Follow the thread #ACCFIT s for a good overview of considerations. #FelllowsFirst #MedEd
How does plasma volume and erythrocyte volume change during pregnancy? 1/12
How does plasma volume and erythrocyte volume change during pregnancy? 1/12
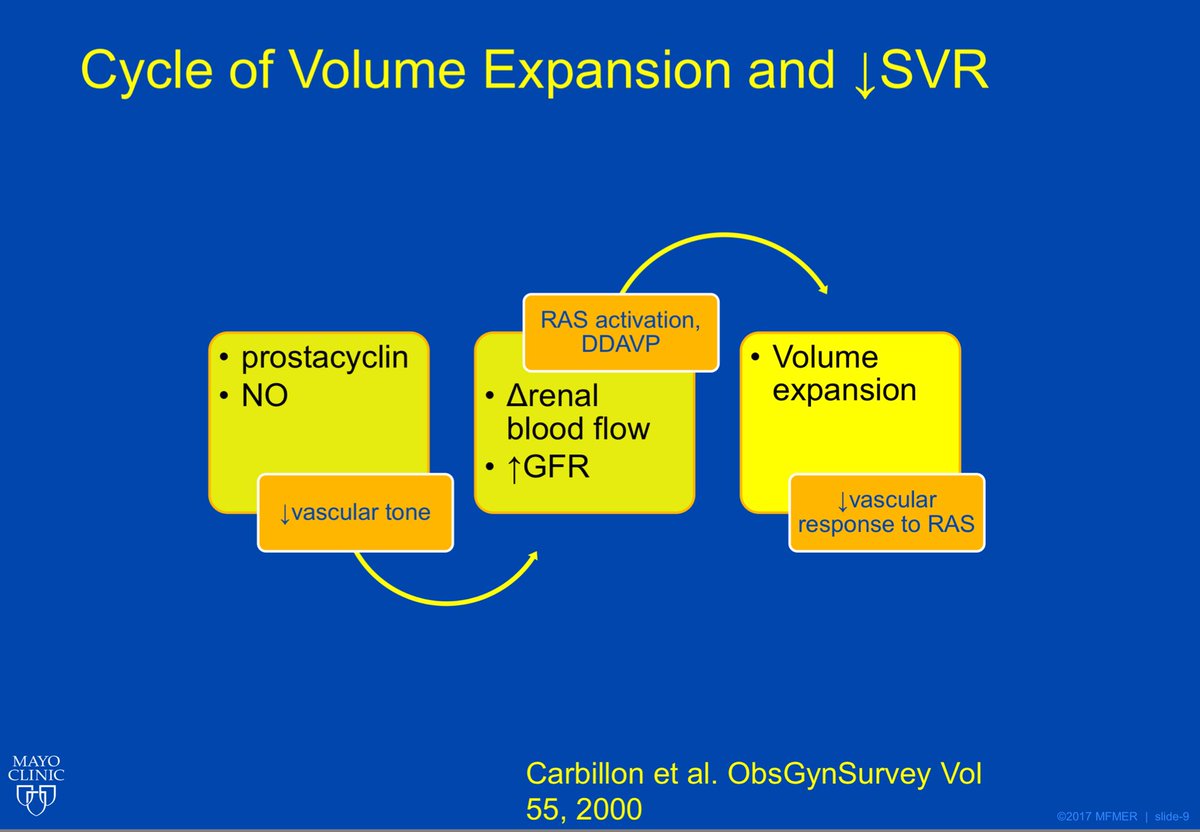
#PregnancyCardiology Primer
Other important factors in the cycle of volume expansion and decreased SVR
2/12
#FellowsFirst #ACCFIT
Other important factors in the cycle of volume expansion and decreased SVR
2/12
#FellowsFirst #ACCFIT



#FITSurvivalGuide: #HeartFailure management — a #tweetorial for #ACCFIT
1️⃣ Non-pharmacologic
2️⃣ Acute HF
3️⃣ Staging
4️⃣ HFrEF
5️⃣ HFpEF
6️⃣ Devices
7️⃣ Advanced Tx
8️⃣ Misc
Resources: @HFSA @ishlt @AHAScience @JACCJournals @HRSonline
1️⃣ Non-pharmacologic
2️⃣ Acute HF
3️⃣ Staging
4️⃣ HFrEF
5️⃣ HFpEF
6️⃣ Devices
7️⃣ Advanced Tx
8️⃣ Misc
Resources: @HFSA @ishlt @AHAScience @JACCJournals @HRSonline
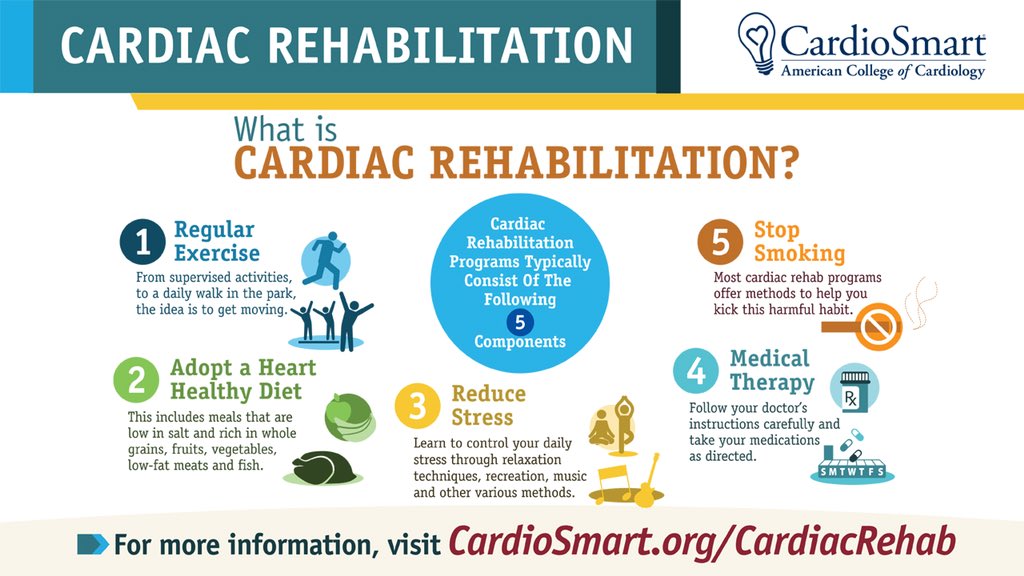
1️⃣ Non-pharmacological therapies for HF:
➖Cardiac rehabilitation can improve functional capacity, exercise duration & mortality
➖Diet: Low Na (2-3 g/day) diet to reduce congestive symptoms
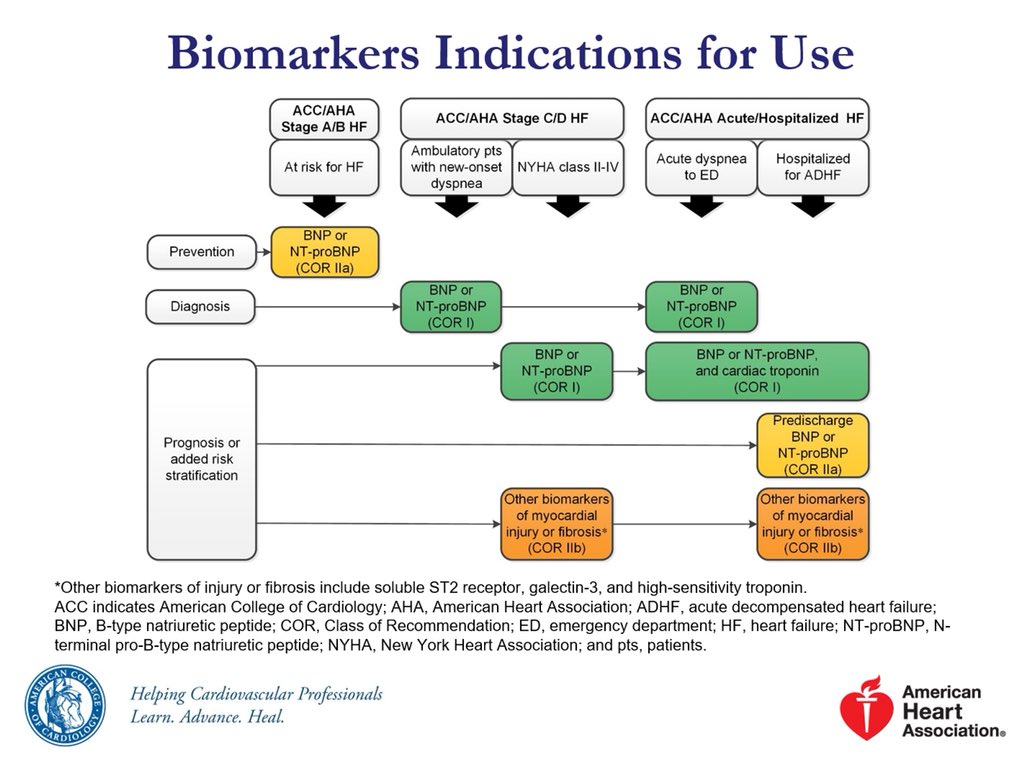
➖Biomarkers have an important role in diagnosis and prognosis of patients with HF
➖Cardiac rehabilitation can improve functional capacity, exercise duration & mortality
➖Diet: Low Na (2-3 g/day) diet to reduce congestive symptoms
➖Biomarkers have an important role in diagnosis and prognosis of patients with HF
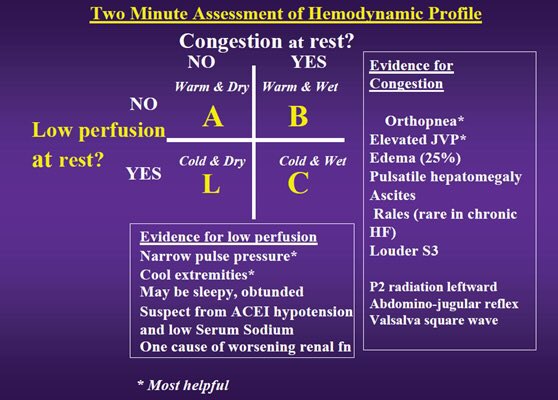
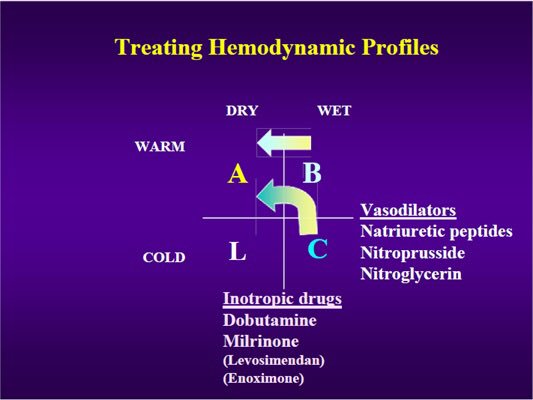
2️⃣ Acute Heart Failure Treatment agenda:
➖ Stabilize condition based on hemodynamics profile
➖ Establish dx, etiology and precipitating factor
➖ Initiate therapy for symptom relief
➖ Preload/afterload reduction
➖ Inhibition of neurohormonal activation for long term mgmt
➖ Stabilize condition based on hemodynamics profile
➖ Establish dx, etiology and precipitating factor
➖ Initiate therapy for symptom relief
➖ Preload/afterload reduction
➖ Inhibition of neurohormonal activation for long term mgmt

#FITSurvivalGuide #ACCFIT
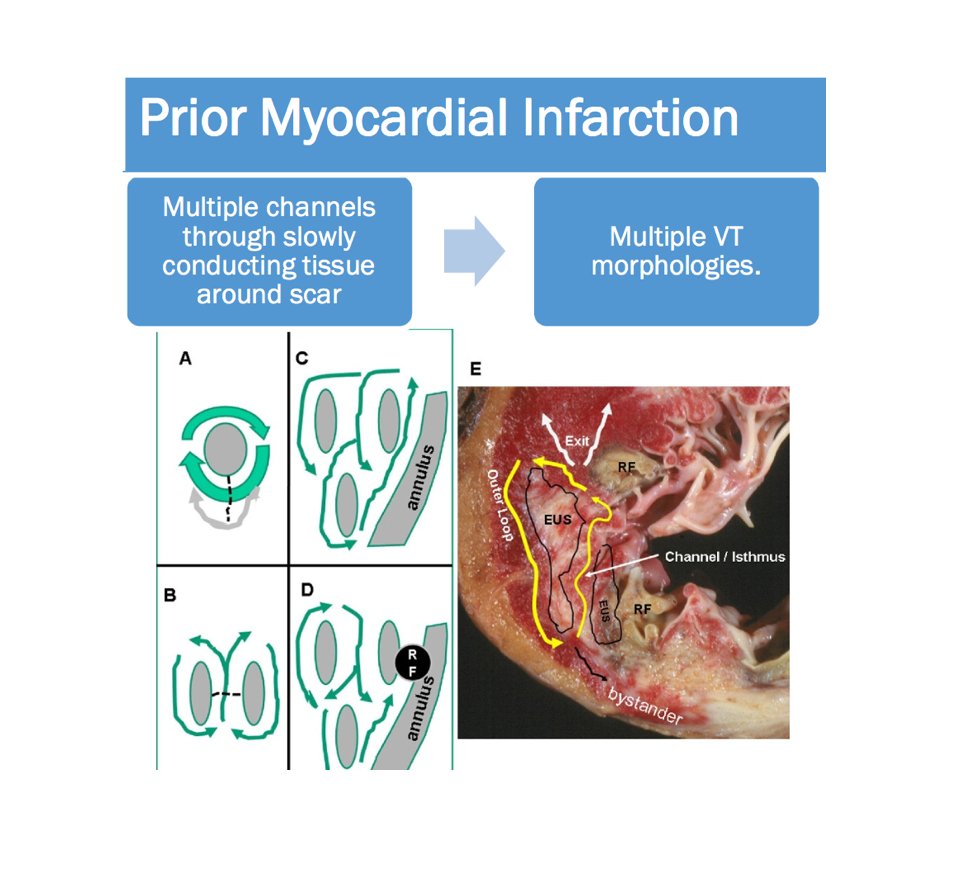
Topic - Ventricular Tachycardia!
Agenda:
1- Approach to evaluating #VT
2- Management of #VT
3- Practice Cases
Please share your thoughts & input to this #tweetorial!
@ACCCardioEd @ACCinTouch #FOAMed @MichiganACC
Topic - Ventricular Tachycardia!
Agenda:
1- Approach to evaluating #VT
2- Management of #VT
3- Practice Cases
Please share your thoughts & input to this #tweetorial!
@ACCCardioEd @ACCinTouch #FOAMed @MichiganACC
#FITSurvivalGuide #ACCFIT
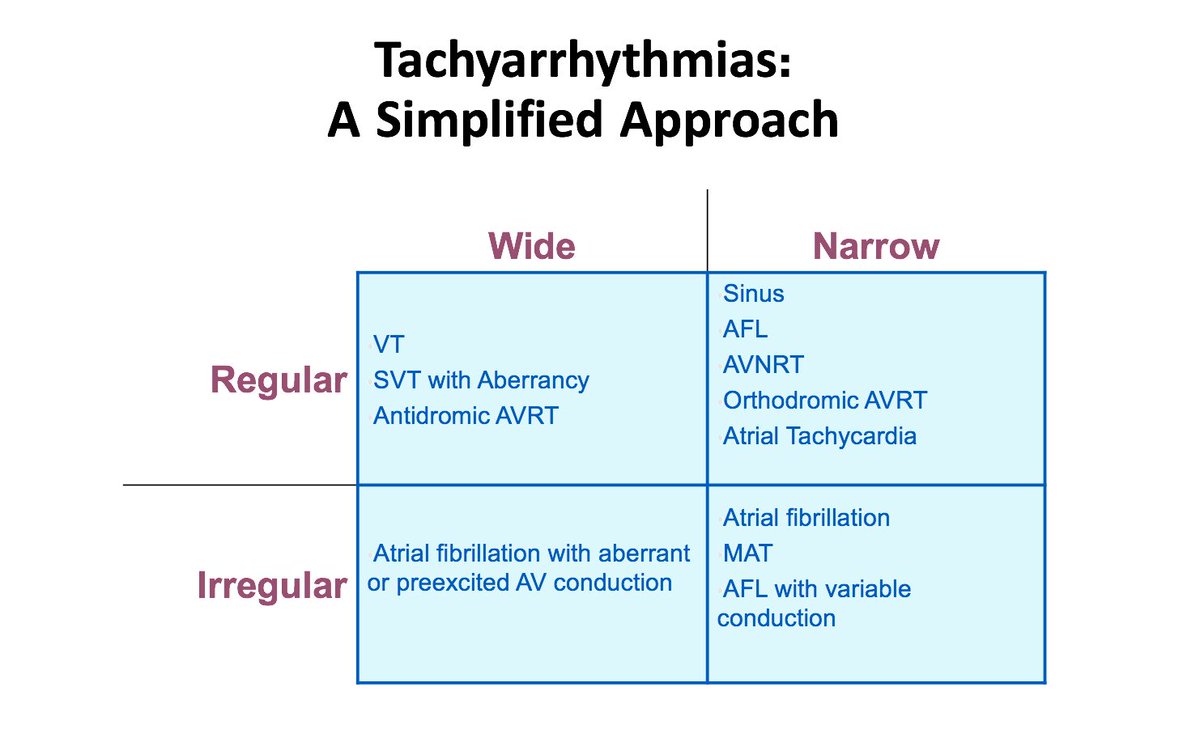
1/10 – Ventricular Tachycardia
Simplified approach to evaluate tachycardia:
Rule #1 – If HD unstable ➡️ shock!
If HD stable, sit down & think.
Step # 1 - QRS: wide or narrow?
Step # 2 - Rhythm: regular or irregular?
This will narrow DDx!
1/10 – Ventricular Tachycardia
Simplified approach to evaluate tachycardia:
Rule #1 – If HD unstable ➡️ shock!
If HD stable, sit down & think.
Step # 1 - QRS: wide or narrow?
Step # 2 - Rhythm: regular or irregular?
This will narrow DDx!
#FITSurvivalGuide #ACCFIT
2/10 - Wide complex tachycardia
Always consider clinical Scenario!
Look for history of MI and cardiomyopathy ➡️ strongly favor #VT!
* If structural heart disease is present, you will be correct 9/10 times with diagnosis of VT!
2/10 - Wide complex tachycardia
Always consider clinical Scenario!
Look for history of MI and cardiomyopathy ➡️ strongly favor #VT!
* If structural heart disease is present, you will be correct 9/10 times with diagnosis of VT!

#FITSurvivalGuide #ACCFIT
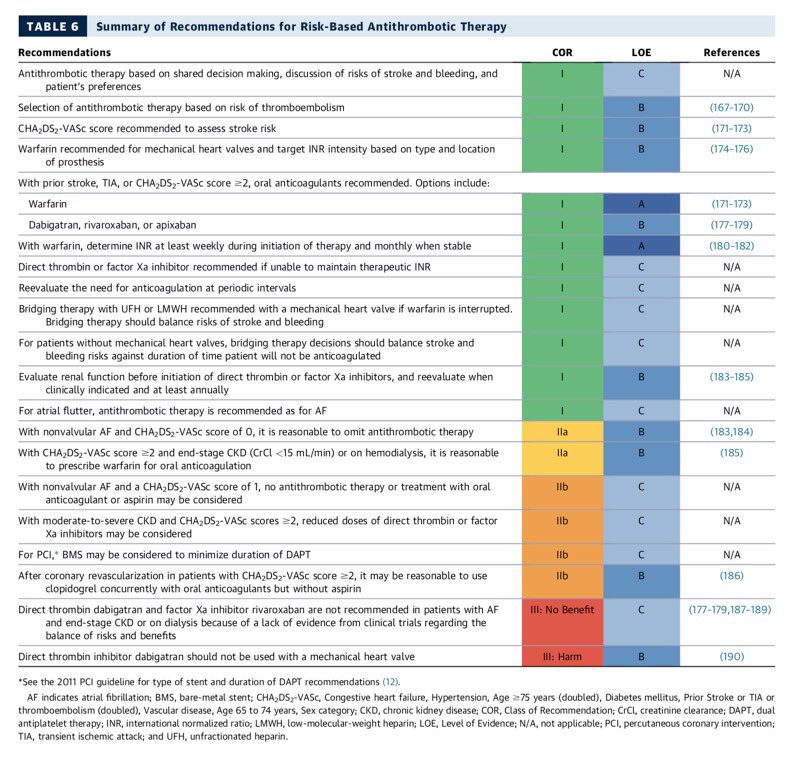
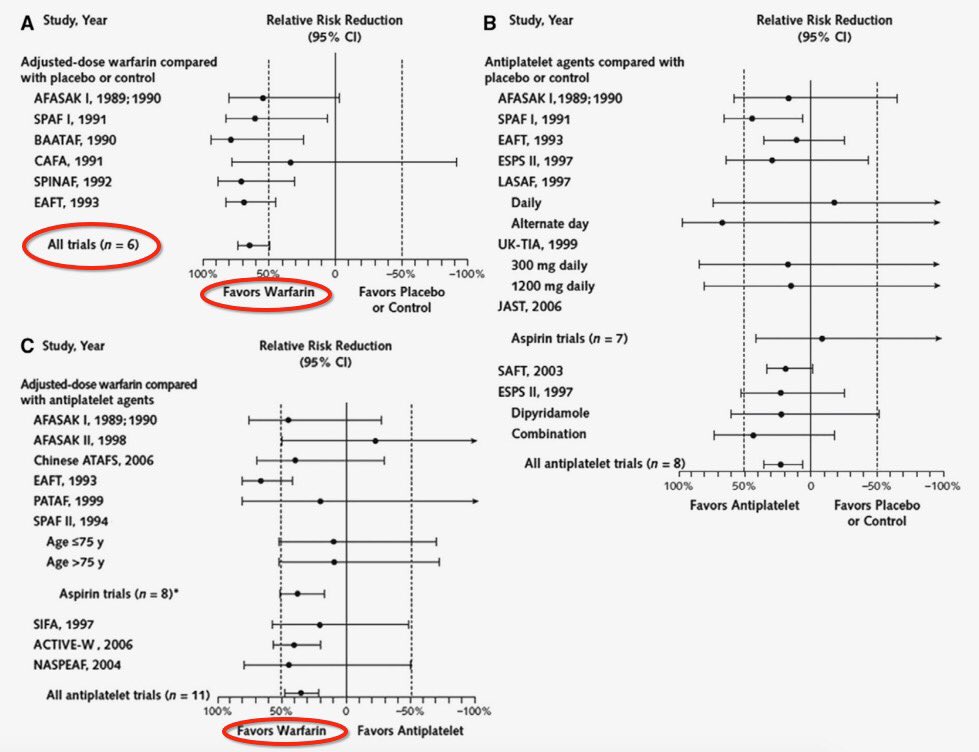
1/10: Stroke🧠 prevention in afib. #warfarin, #noacs, & LAA occlusion devices.
◽️shared decision making is key 🔑
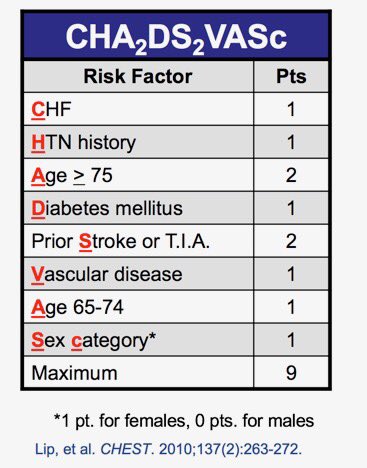
◽️CHADS-Vasc to stratify risk
◽️factor 💸and CrCl 🚽
◽️DAPT+AC= ↑↑bleeding
1/10: Stroke🧠 prevention in afib. #warfarin, #noacs, & LAA occlusion devices.
◽️shared decision making is key 🔑
◽️CHADS-Vasc to stratify risk
◽️factor 💸and CrCl 🚽
◽️DAPT+AC= ↑↑bleeding

2/10
For a quick review on coagulation physiology as it pertains to AC see 📽below.
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD @majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza
@SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm
For a quick review on coagulation physiology as it pertains to AC see 📽below.
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD @majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza
@SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm
3/10
Warfarin 🐀☣️
◽️interferes with normal post translational gamma-carboxylation of vitamin K dependent clotting factors 2️⃣7️⃣9️⃣🔟
◽️doesn’t inactivate functional clotting factors
◽️prothrombin half life: 72h
◽️Ergo INR effect 24-36 hr
🛑 teratogenic
Warfarin 🐀☣️
◽️interferes with normal post translational gamma-carboxylation of vitamin K dependent clotting factors 2️⃣7️⃣9️⃣🔟
◽️doesn’t inactivate functional clotting factors
◽️prothrombin half life: 72h
◽️Ergo INR effect 24-36 hr
🛑 teratogenic

#FITSurvivalGuide #ACCFIT
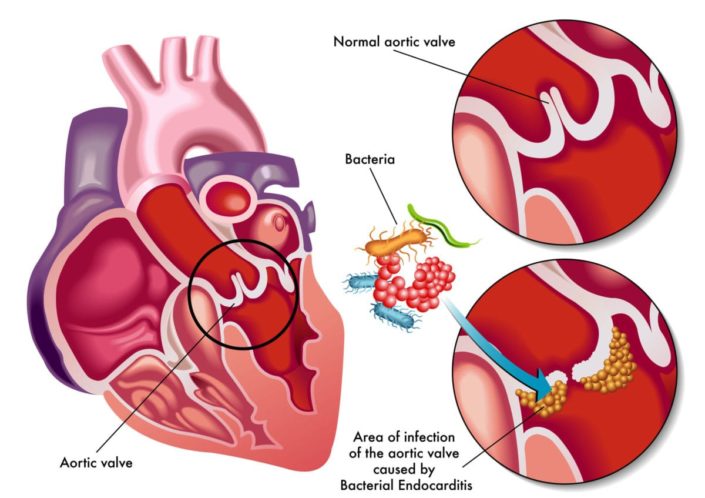
#InfectiveEndocarditis.
1/10 Not comprehensive. ⬇️⬇️some imp. points. Hx, exam, echo, micro data essential to diagnose & treat apporpriately. Suggested read : 2014 ACC/AHA valve guideline with 2017 Focused update.
cc: @dr_chirumamilla
#InfectiveEndocarditis.
1/10 Not comprehensive. ⬇️⬇️some imp. points. Hx, exam, echo, micro data essential to diagnose & treat apporpriately. Suggested read : 2014 ACC/AHA valve guideline with 2017 Focused update.
cc: @dr_chirumamilla
2/10
Incidence varies. Native IE 10-15/100K/year, PVE ~30% of all IE.
Risk ⬆️>60 years, ♂️sex, IV drug use, HIV, hemodialysis, poor 🦷 with infection, Alcoholic cirrhosis, intravascular device, CIED, immunosuppression, Transplants, Rheumatic ❤️ dz...
Incidence varies. Native IE 10-15/100K/year, PVE ~30% of all IE.
Risk ⬆️>60 years, ♂️sex, IV drug use, HIV, hemodialysis, poor 🦷 with infection, Alcoholic cirrhosis, intravascular device, CIED, immunosuppression, Transplants, Rheumatic ❤️ dz...


3/10
-Vegetations - "On the lower pressure side of a cardiac chamber / structural lesion or at site of impact of high-velocity blood jets "
-Acute vs Subacute IE
-Right vs Left sided IE
-Early (<60 days) vs Late ( >60days) Prosthetic IE
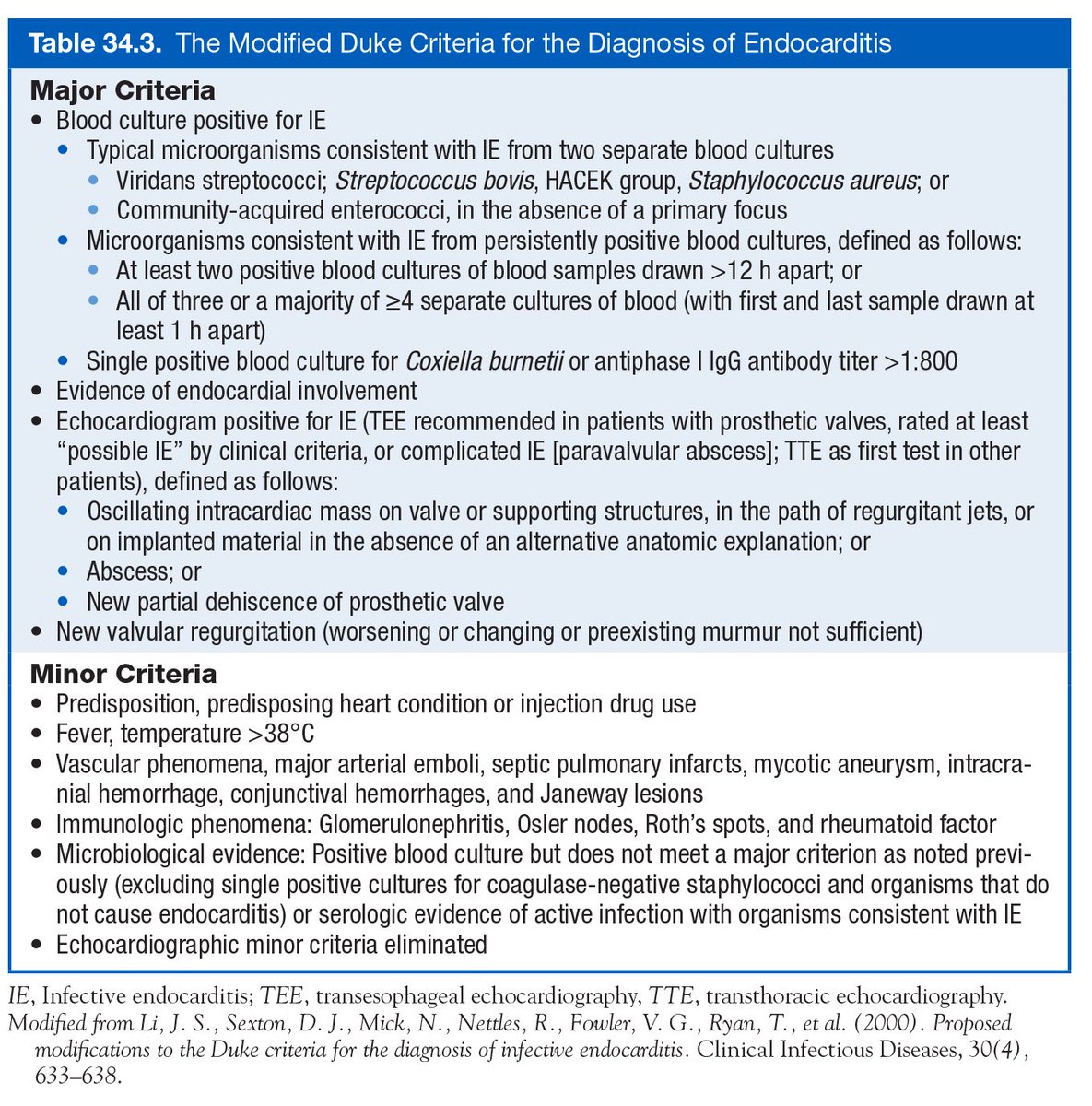
⭐️Modified Duke's criteria⭐️
-Vegetations - "On the lower pressure side of a cardiac chamber / structural lesion or at site of impact of high-velocity blood jets "
-Acute vs Subacute IE
-Right vs Left sided IE
-Early (<60 days) vs Late ( >60days) Prosthetic IE
⭐️Modified Duke's criteria⭐️




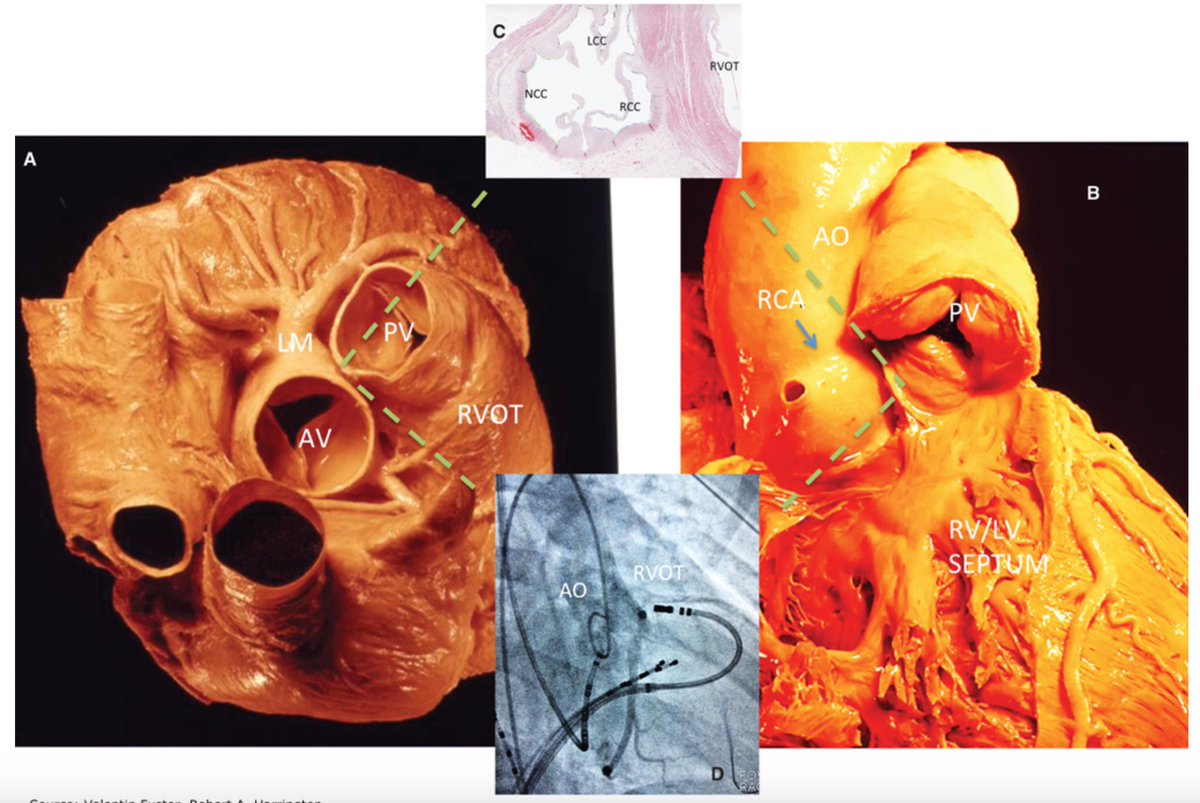
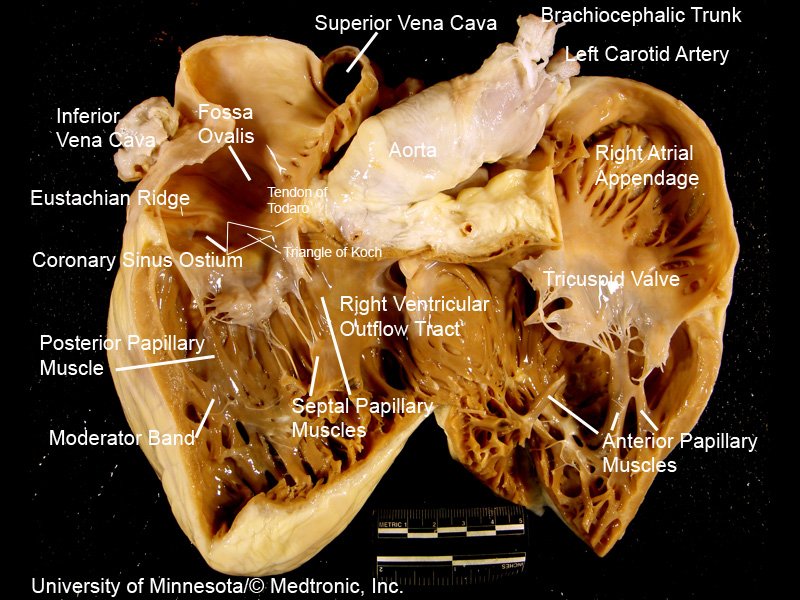
#FITSurvivalGuide: The Forgotten Valve-#TricuspidRegurgitation (#TR) #tweetorial for the new #ACCFIT!
1⃣ Anatomy
2⃣ Etiologies
3⃣ Classification
4⃣ Diagnosis
5⃣ Treatment
Resources: @ASE360 @JACCJournals @CircAHA @ACCCardioEd @UMNews @Medtronic
1/10
cc: @dr_chirumamilla
1⃣ Anatomy
2⃣ Etiologies
3⃣ Classification
4⃣ Diagnosis
5⃣ Treatment
Resources: @ASE360 @JACCJournals @CircAHA @ACCCardioEd @UMNews @Medtronic
1/10
cc: @dr_chirumamilla
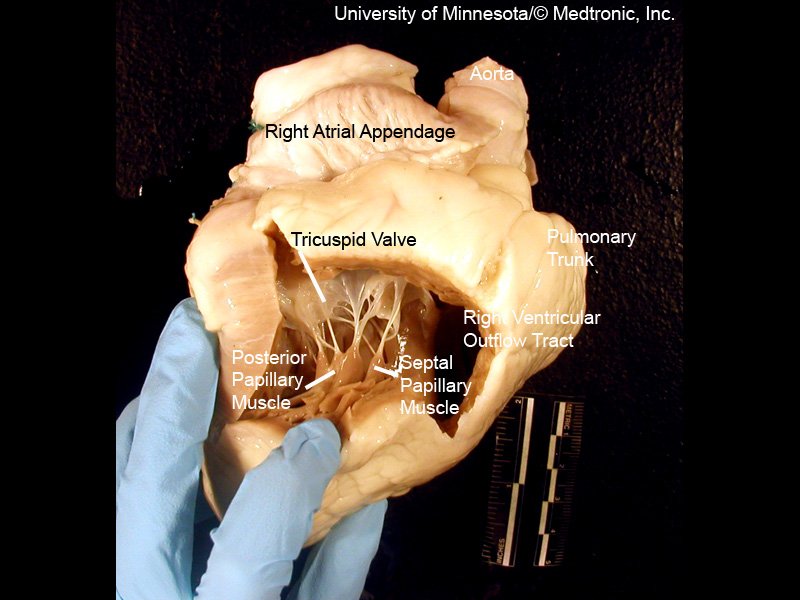
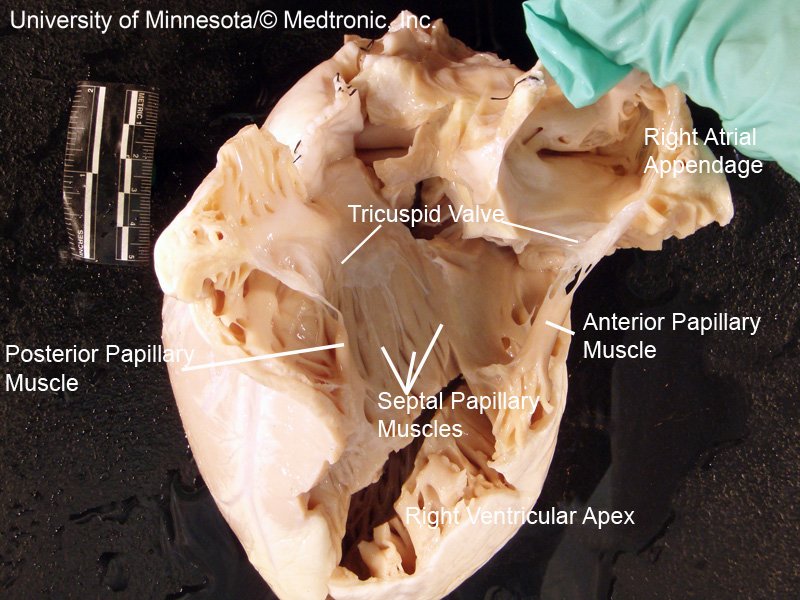
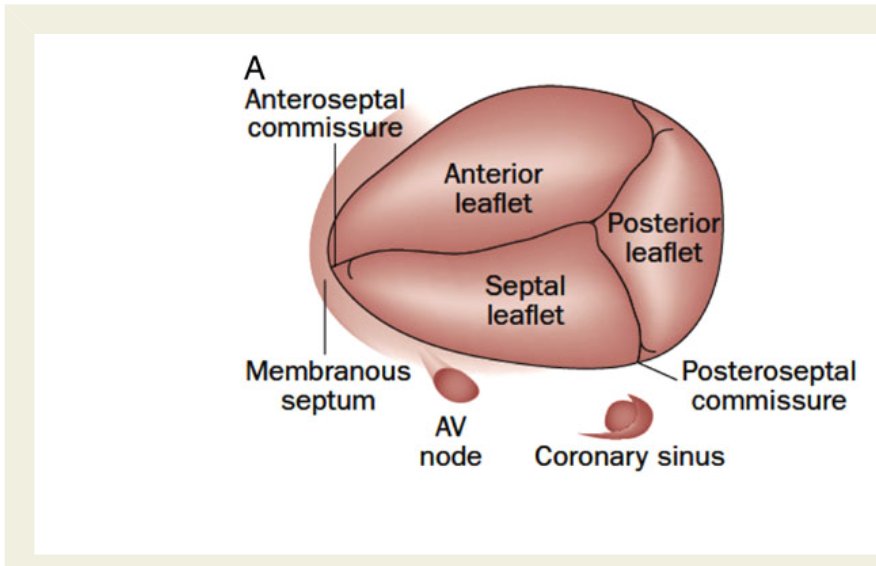
[2/10] Impt to understand #TricuspidValve 1⃣ Anatomy
3 leaflets ⬇️ + fibrous annulus + 2 papillary 💪🏽 + chordae tendinae + RA/RV ❤️
⬛️ Anterior 🍃 (largest)
◾️Posterior
▪️Septal (smallest)
(note: throughout #tweetorial, see image descriptions for more content)
3 leaflets ⬇️ + fibrous annulus + 2 papillary 💪🏽 + chordae tendinae + RA/RV ❤️
⬛️ Anterior 🍃 (largest)
◾️Posterior
▪️Septal (smallest)
(note: throughout #tweetorial, see image descriptions for more content)
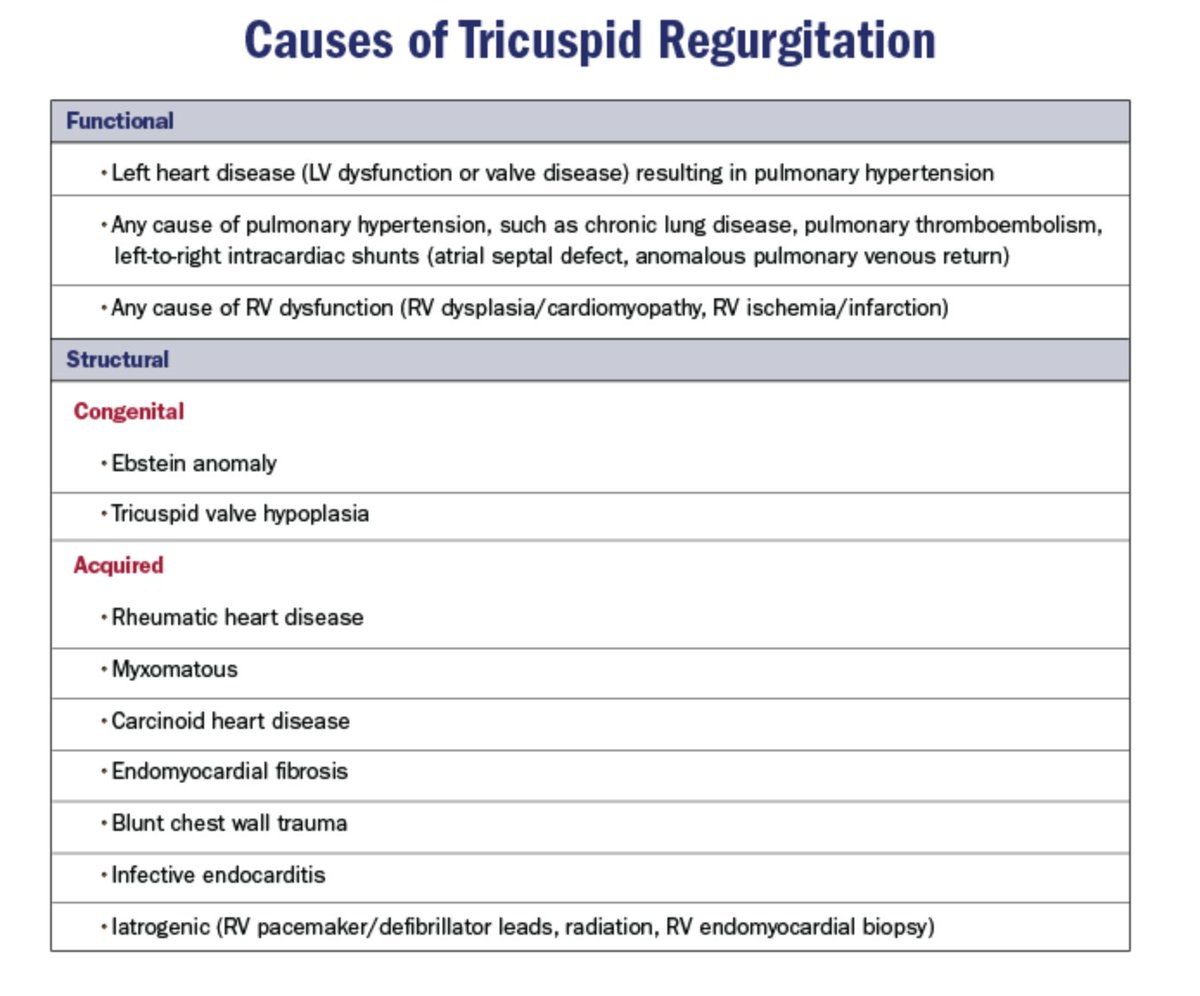
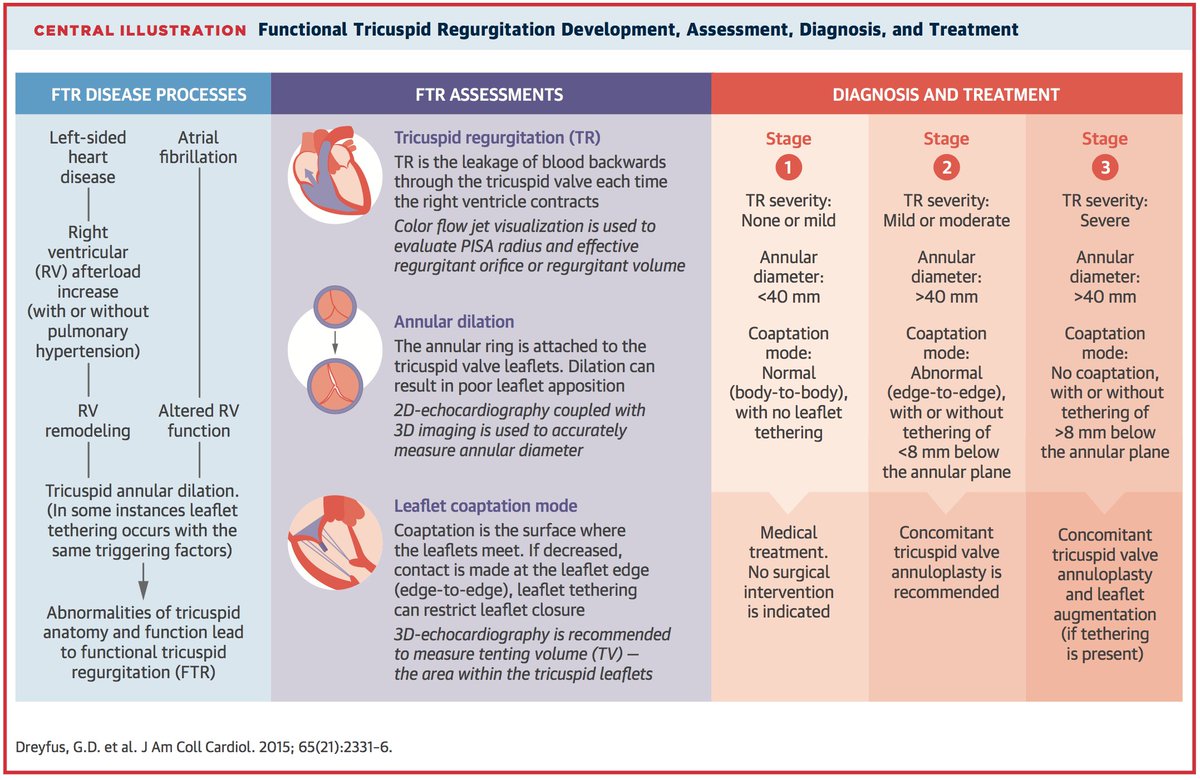
[3/10] 2⃣ Etiologies = Structural (1º) vs. Functional (FTR)
Keep chart ⬇️ DDx in mind when reading #EchoFirst
~80% of significant TR = FTR/2º to TA dilatation + leaflet tethering ⬅️ RV remodeling ⬅️ volume and/or pressure overload
Structural (1º) cause = less common
Keep chart ⬇️ DDx in mind when reading #EchoFirst
~80% of significant TR = FTR/2º to TA dilatation + leaflet tethering ⬅️ RV remodeling ⬅️ volume and/or pressure overload
Structural (1º) cause = less common

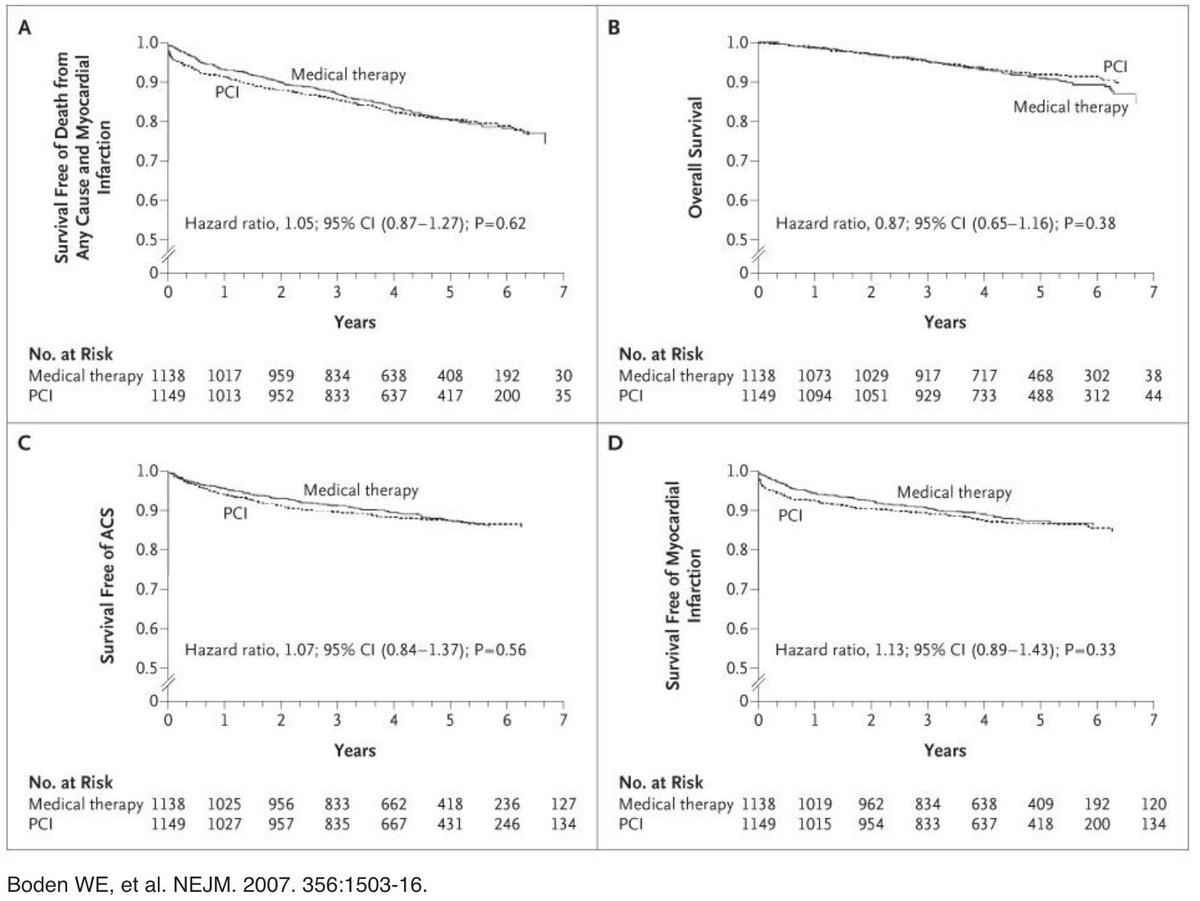
1/10 “To PCI, or Not to PCI, That is the Question” Will Shakespeare, MD
#FITSurvivalGuide
*Per many contentious #cardiotwitter discussions I realize this is loaded topic but I’m going to attempt an early stage #ACCFIT overview while recognizing there is a lot of nuance.
#FITSurvivalGuide
*Per many contentious #cardiotwitter discussions I realize this is loaded topic but I’m going to attempt an early stage #ACCFIT overview while recognizing there is a lot of nuance.

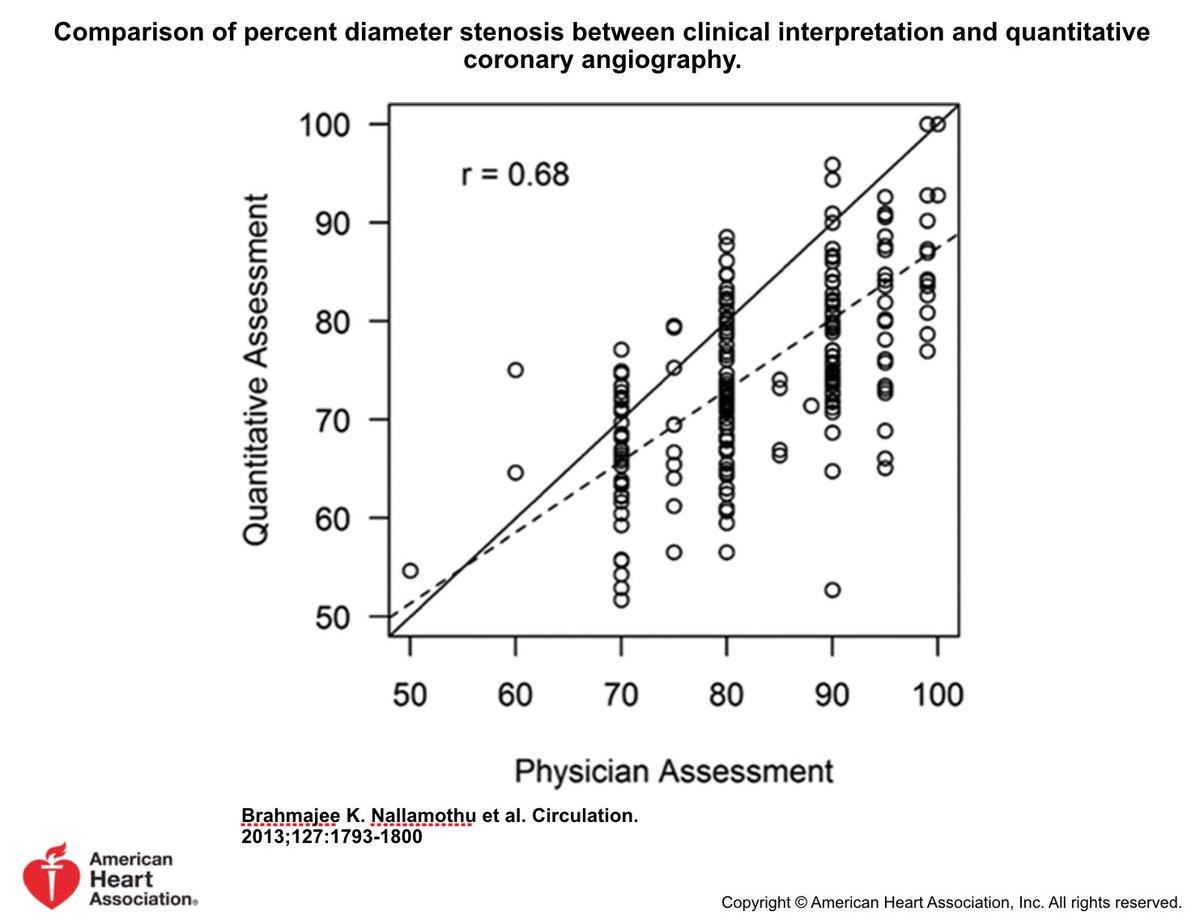
2/10 Why not “See lesion Fix lesion”?
Poor correlation between est'd visual stenosis & quantitative stenosis. And, without noninvasive ischemic data, coronary angio has limited accuracy w/ regard to identifying significance of many stenoses
*STEMI PCI already done @KhandelwalMD
Poor correlation between est'd visual stenosis & quantitative stenosis. And, without noninvasive ischemic data, coronary angio has limited accuracy w/ regard to identifying significance of many stenoses
*STEMI PCI already done @KhandelwalMD
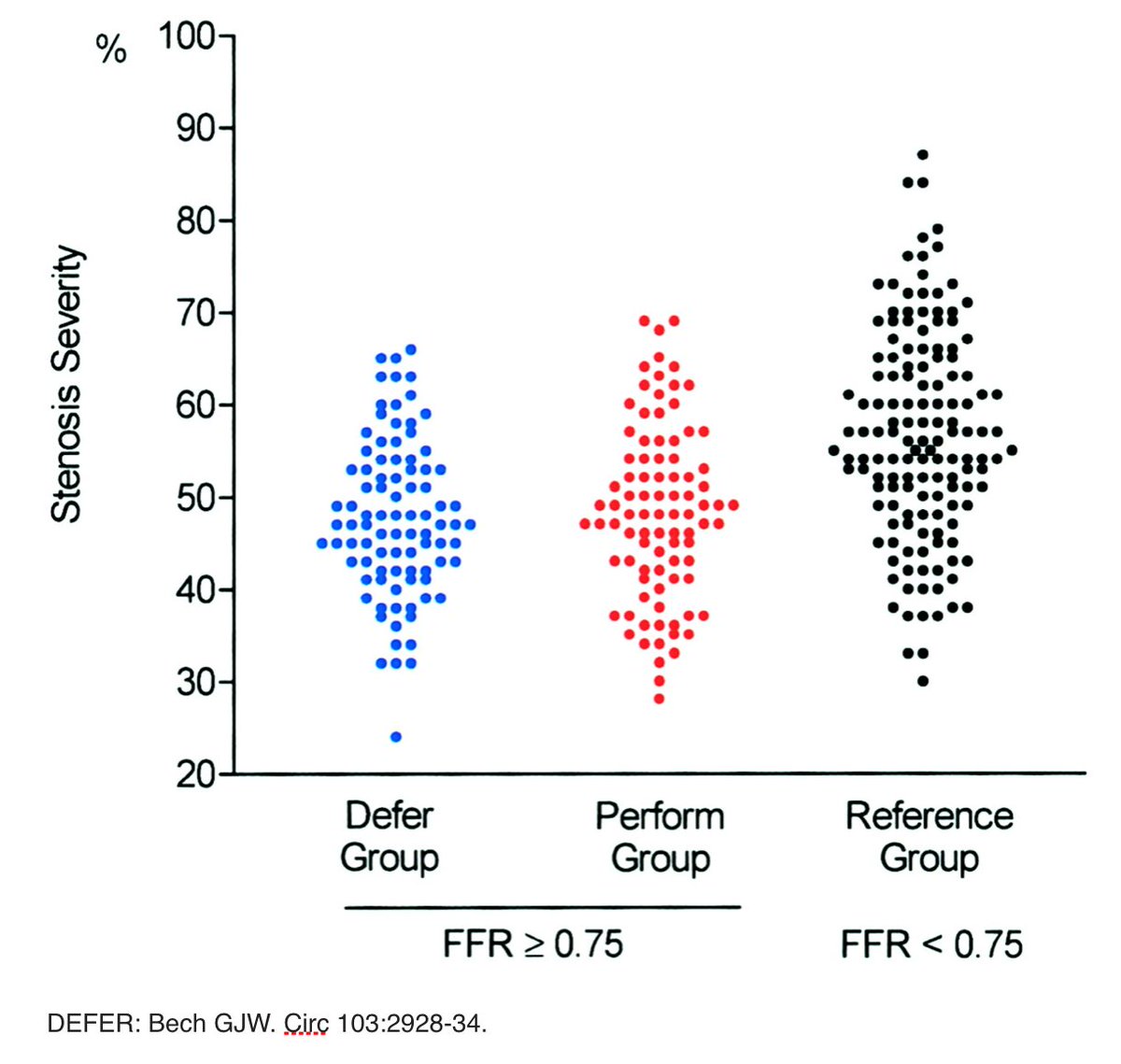
3/10 COURAGE trial (OMT vs OMT and PCI of visually-estimated significant stenoses): No difference death/MI between OMT & OMT/PCI. PCI demonstrated clinical benefit only when treating relevant myocardial ischemia determined by noninvasive testing.


Intro/10 #STEMI #tweetorial #FITSurvivalGuide for #ACCFIT. Organized by @dr_chirumamilla. @ACCCardioEd @ACCinTouch
1/10 #STEMI from ruptured plaque, less plaque erosion. @BraunwaldEugene pic demonstrates LDL oxidized, glycated➡️cytokines release express adhesion molecules➡️monocytes roll, diapedesis➡️ingest LDL, become foam cell➡️SMC migrate, proliferate➡️some apoptosis➡️plaque



1/
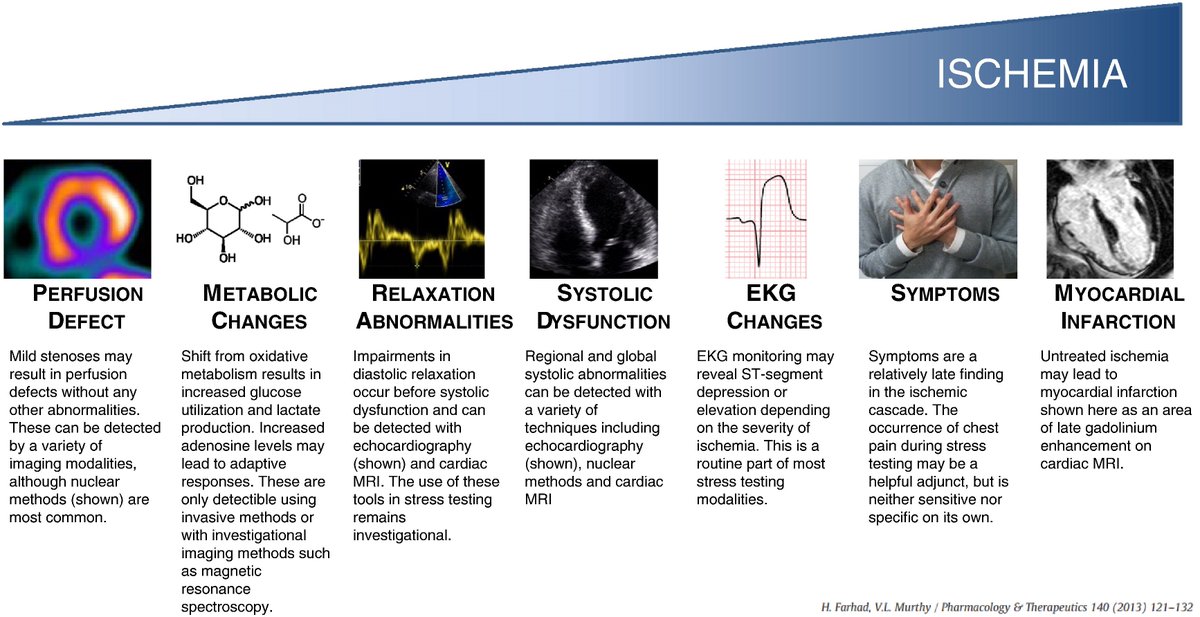
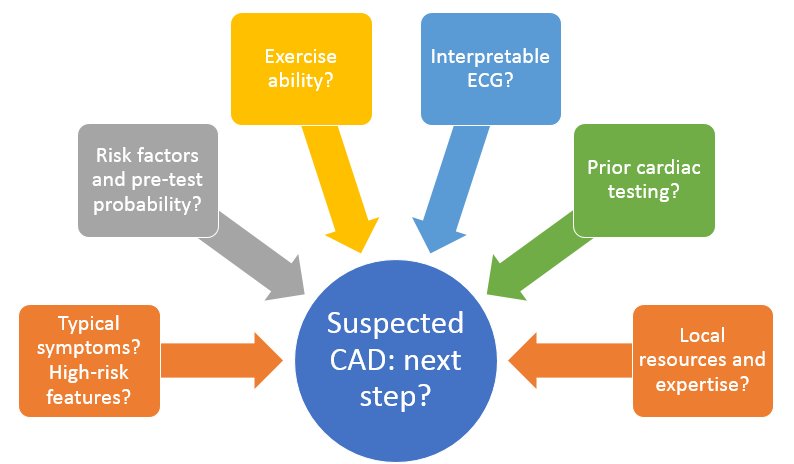
Let’s continue with Day 7 of the cardiology #FITSurvivalGuide #tweetorial! Today we will talk about basics of stress testing for diagnosing CAD.
#ACCFIT #CardioMedEd #FOAMed @ACCinTouch @ACCCardioEd
Let’s continue with Day 7 of the cardiology #FITSurvivalGuide #tweetorial! Today we will talk about basics of stress testing for diagnosing CAD.
#ACCFIT #CardioMedEd #FOAMed @ACCinTouch @ACCCardioEd
2/
Let’s start with a case: 55 y/o woman with CV risk factors presents to clinic with mild CP for 3 months. What is the next test if you want to diagnose significant CAD?
Let’s start with a case: 55 y/o woman with CV risk factors presents to clinic with mild CP for 3 months. What is the next test if you want to diagnose significant CAD?
3/
Not enough info. History/physical critical. Starting meds ok but get a diagnosis if case not clear cut. Exercise testing is better but not appropriate for every patient. Cath first if you believe unstable/high-risk disease or if symptomatic + high-pretest probability.
Not enough info. History/physical critical. Starting meds ok but get a diagnosis if case not clear cut. Exercise testing is better but not appropriate for every patient. Cath first if you believe unstable/high-risk disease or if symptomatic + high-pretest probability.
Kicking off #3TBigSky18 at #CVBigSky with @ShashankSinhaMD talking about public speaking @ACCCardioEd @keaglemd @mwcullen @craigalpert #ACCFIT

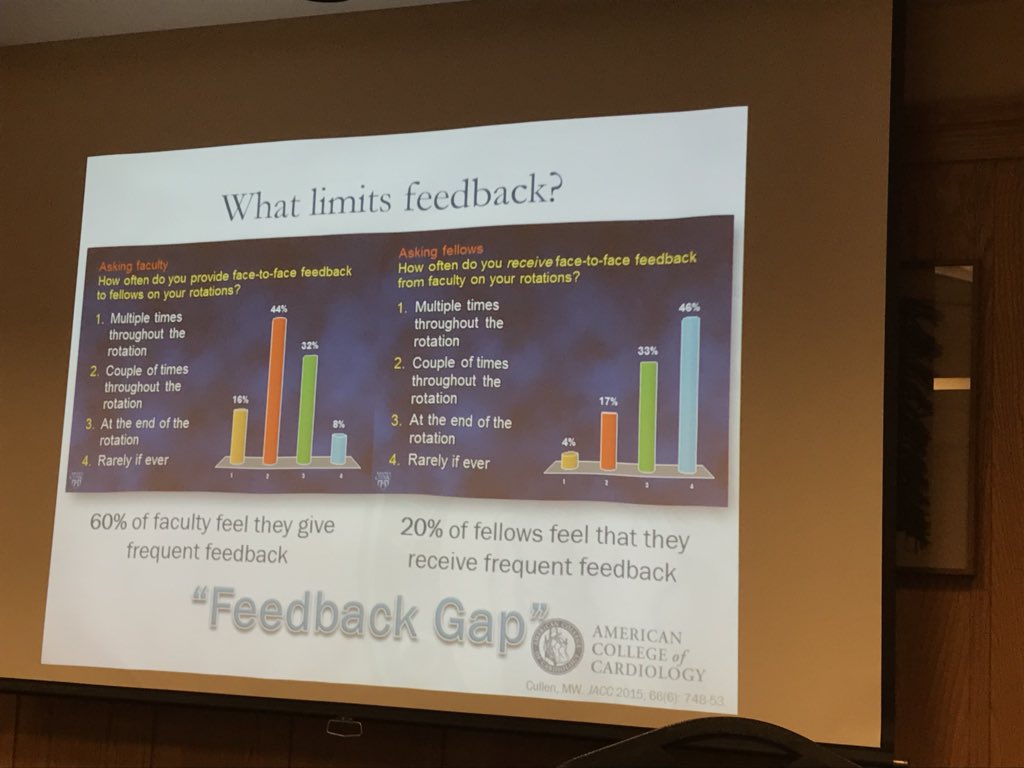
@mwcullen discusses how perception of feedback in #MedEd matters #3TBigSky18 #CVBigSky #ACCFIT @ACCCardioEd @ShashankSinhaMD @craigalpert
PowerPoint theory with @craigalpert #3TBigSky18 #CVBigSky #ACCFIT @ACCCardioEd @ShashankSinhaMD @mwcullen