Discover and read the best of Twitter Threads about #TR
Most recents (1)

#FITSurvivalGuide: The Forgotten Valve-#TricuspidRegurgitation (#TR) #tweetorial for the new #ACCFIT!
1⃣ Anatomy
2⃣ Etiologies
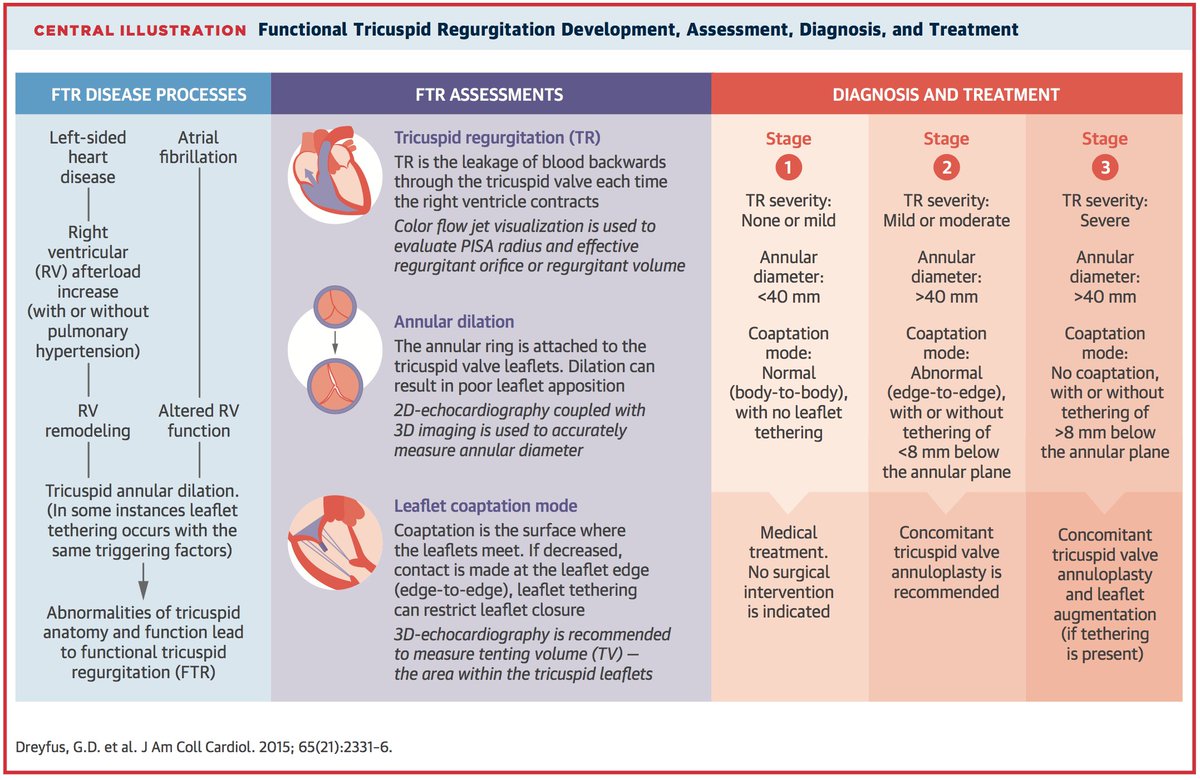
3⃣ Classification
4⃣ Diagnosis
5⃣ Treatment
Resources: @ASE360 @JACCJournals @CircAHA @ACCCardioEd @UMNews @Medtronic
1/10
cc: @dr_chirumamilla
1⃣ Anatomy
2⃣ Etiologies
3⃣ Classification
4⃣ Diagnosis
5⃣ Treatment
Resources: @ASE360 @JACCJournals @CircAHA @ACCCardioEd @UMNews @Medtronic
1/10
cc: @dr_chirumamilla
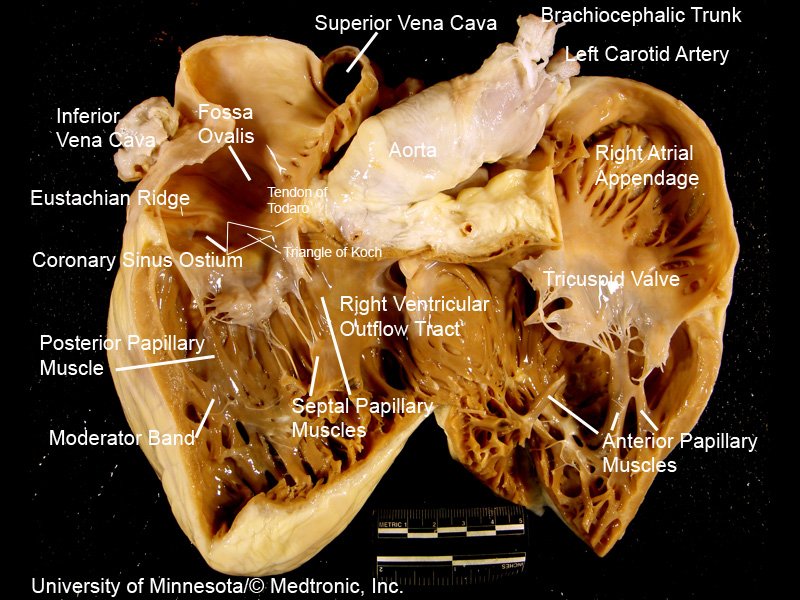
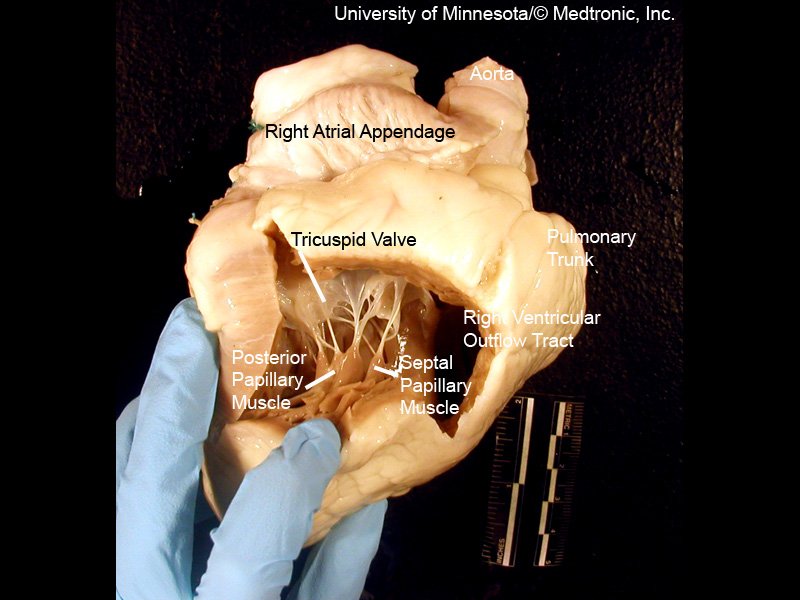
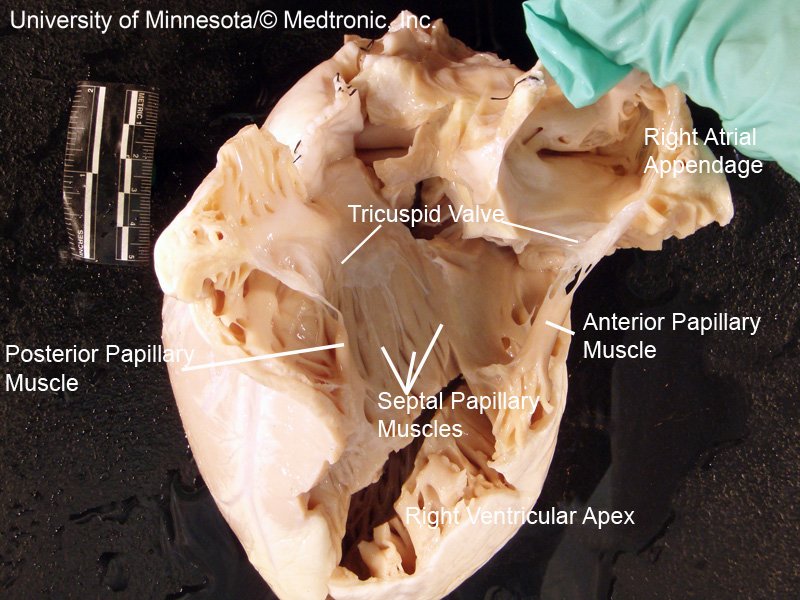
[2/10] Impt to understand #TricuspidValve 1⃣ Anatomy
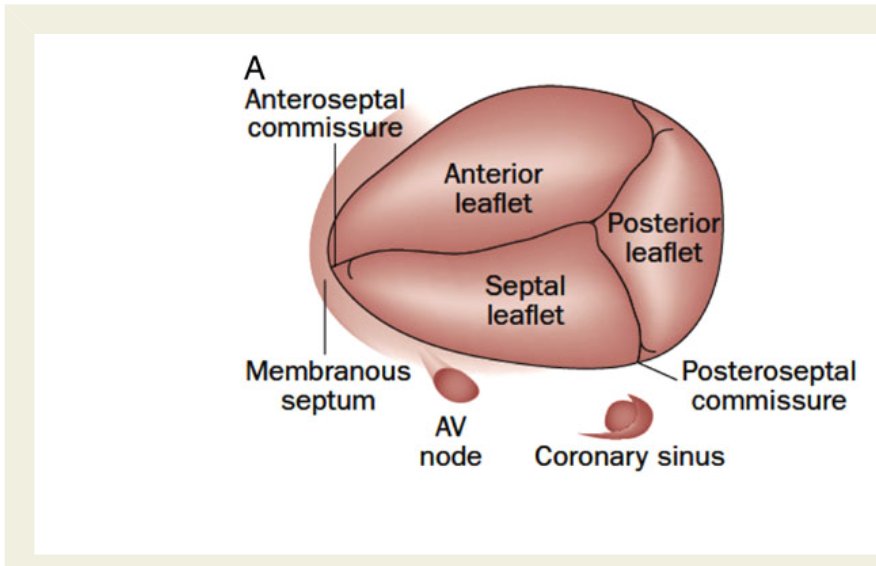
3 leaflets ⬇️ + fibrous annulus + 2 papillary 💪🏽 + chordae tendinae + RA/RV ❤️
⬛️ Anterior 🍃 (largest)
◾️Posterior
▪️Septal (smallest)
(note: throughout #tweetorial, see image descriptions for more content)
3 leaflets ⬇️ + fibrous annulus + 2 papillary 💪🏽 + chordae tendinae + RA/RV ❤️
⬛️ Anterior 🍃 (largest)
◾️Posterior
▪️Septal (smallest)
(note: throughout #tweetorial, see image descriptions for more content)
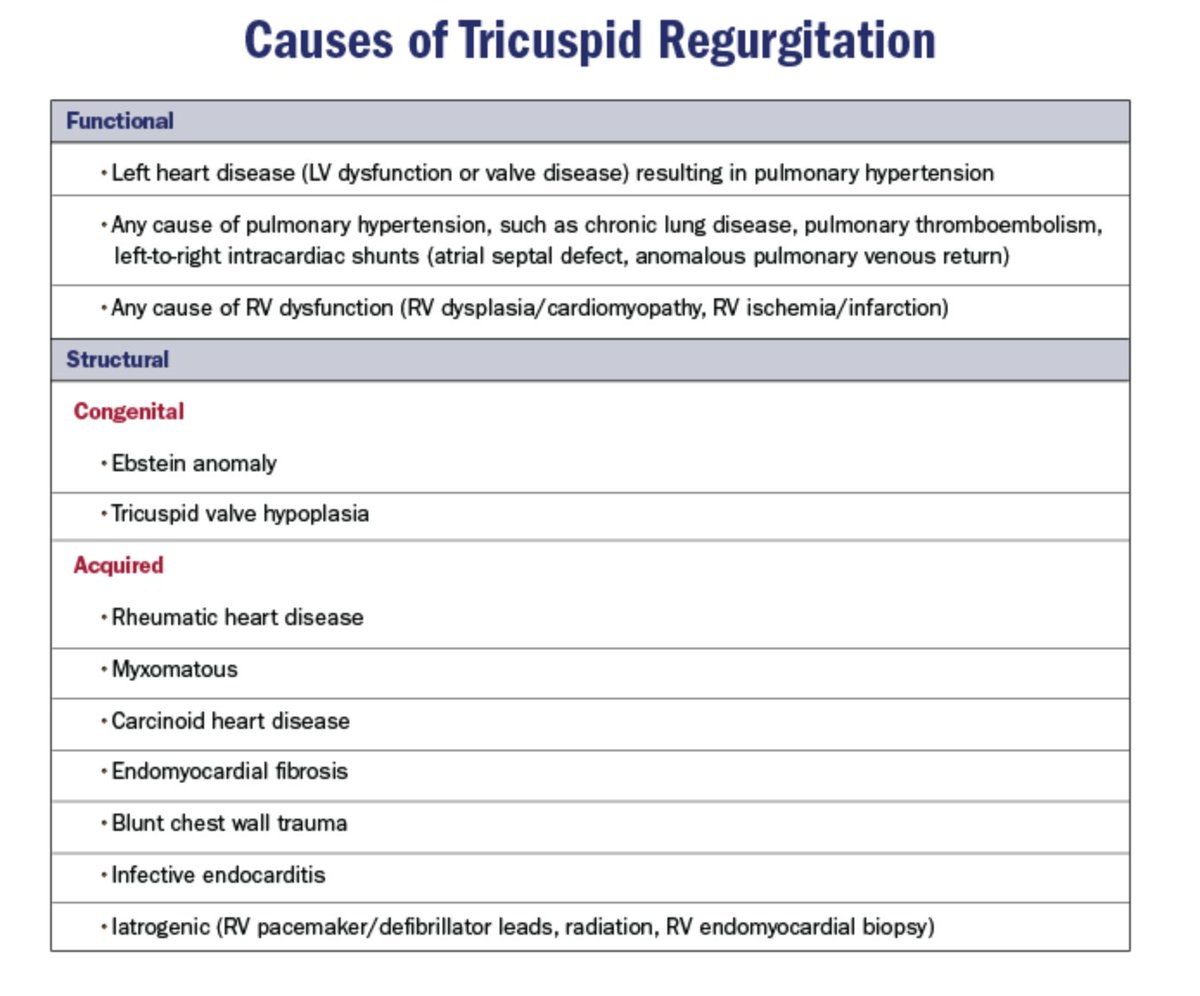
[3/10] 2⃣ Etiologies = Structural (1º) vs. Functional (FTR)
Keep chart ⬇️ DDx in mind when reading #EchoFirst
~80% of significant TR = FTR/2º to TA dilatation + leaflet tethering ⬅️ RV remodeling ⬅️ volume and/or pressure overload
Structural (1º) cause = less common
Keep chart ⬇️ DDx in mind when reading #EchoFirst
~80% of significant TR = FTR/2º to TA dilatation + leaflet tethering ⬅️ RV remodeling ⬅️ volume and/or pressure overload
Structural (1º) cause = less common