THREAD: Yeah, I have insomnia, so here’s some wonky info re. single payer, M4A and the Michigan Gubernatorial primary. 1/
2/ Now that the #MIGov primary is over, since the most contentious debate between El-Sayed and Whitmer (besides 'dark money') was about single-payer healthcare, let's get a few things straight:
3/ 1. "Single Payer" refers to any healthcare system where the gov’t is the payment source for healthcare providers (doctors/hospitals/drug cos/etc).
4/ Most single payer plans still require *some* level of out-of-pocket payment by enrollees…including Medicare, which DOES include premiums, deductibles and co-pays.
5/ 2. "Pure" Single Payer--which is what both Abdul's "MichCare" plan (at the state level) and Bernie's "M4A" plan (at the federal level) would entail—means that there's ZERO out of pocket cost to the enrollee/patient; EVERYTHING is paid for by the government & funded via taxes.
6/ 3. It could be argued that "MichCare" would actually be a *dual*-payer system since it'd be funded partly by the feds and partly by the state, like Medicaid is today...but the "single" part refers to who pays the *providers*.
7/ Since they'd only be paid by the state of Michigan (which would in turn be reimbursed by the federal government), it would still qualify as "single payer".
8/ 4. "Universal Coverage" is NOT THE SAME THING as "single payer". Universal Coverage refers to any healthcare system in which 100% of the population is covered by it.
9/ 5. "Single Payer" does NOT necessarily mean "Comprehensive". Canada doesn't cover dental care, vision care, prescription medications, psychotherapists or physical therapy, for instance. It may cover 100% of everything else…but it doesn’t cover ANY of those things.
10/ 6. Most industrialized nations DO have Universal Coverage (UC) but very few actually have Single Payer (SP). Canada, South Korea and Taiwan are the only countries I know of which have Universal Single Payer (USP), and again, that doesn't mean they're Comprehensive.
11/ 7. It's impossible to have "Medicare for All" at the state level, since Medicare is a FEDERAL program. You can certainly have a "Medicare-like SP program", but it isn't Medicare. In fact, many progressive healthcare wonks think *Medicaid* for All would make more sense.
12/ 8. This one is Michigan-specific: In terms of Abdul's "MichCare" proposal, regardless of the logistics/mechanics of how it would work if it actually became law, here's the realities of what would be required—I’m NOT making a judgement about the feasibility of any of these:
13/ a) obviously it would first have to pass the state House, Senate and be signed by the Governor;
b) the state Constitution would have to be altered to allow for the progressive income/payroll tax;
b) the state Constitution would have to be altered to allow for the progressive income/payroll tax;
14/ c) the Centers for Medicare & Medicaid (CMS) Administrator, appointed by the President, would have to approve of waivers allowing all federal Medicare, Medicaid, CHIP and ACA funding to be redirected towards the new state program.
15/ Keep in mind that if FEDERAL funding for Medicare, Medicaid, CHIP or the ACA (completely outside of the Governor/state legislature’s control) is messed with, it screws with the healthcare coverage for EVERYONE in that state, not “just” those previously on Medicaid/ACA plans.
16/ Don’t get me wrong, there’s a huge *upside* to that as well, since it makes it more politically dangerous when the entire state population is at risk instead of only a small sliver…but it’s something to take into consideration.
17/ 9. If you've read this whole thread and thought to yourself "eh, he's splitting hairs over piddly details!",
congratulations: You're part of the problem. Those "piddly details" are at the HEART of the debate over how to proceed with the next steps in healthcare policy.
congratulations: You're part of the problem. Those "piddly details" are at the HEART of the debate over how to proceed with the next steps in healthcare policy.
18/ 10. Put another way: Healthcare policy is complicated.
/END
P.S. I rely in part on individual supporters. If you find my work of value & are in a position to do so, please consider chipping in, thank you!
acasignups.net/donate
/END
P.S. I rely in part on individual supporters. If you find my work of value & are in a position to do so, please consider chipping in, thank you!
acasignups.net/donate
19. ADDENDUM: Earlier I said only 3 Nations have true Single Payer systems. What about the United Kingdom? Well, they actually have Socialized Medicine, which goes well BEYOND Single Payer. Not only is payment handled almost entirely through the government, so are providers.
20/ That is, in the UK the doctors generally work directly for the government and the hospitals are owned/run by it. There’s a few exceptions, I believe. Closest equivalent we have here in the U.S. is the Veterans Administration. Like every other system, there are tradeoffs.
21/ I strongly recommend reading this “NCAA Final Four” style comparison of different healthcare systems by @aaronecarroll and @afrakt for further insight into the tradeoffs involved: nytimes.com/interactive/20…
@aaronecarroll @afrakt 22/ Since this thread has received some attention, I’ll add a few more points…
This is one of the most important survey results Democrats should be looking at on healthcare right now:
acasignups.net/18/03/27/whoa-…
This is one of the most important survey results Democrats should be looking at on healthcare right now:
acasignups.net/18/03/27/whoa-…
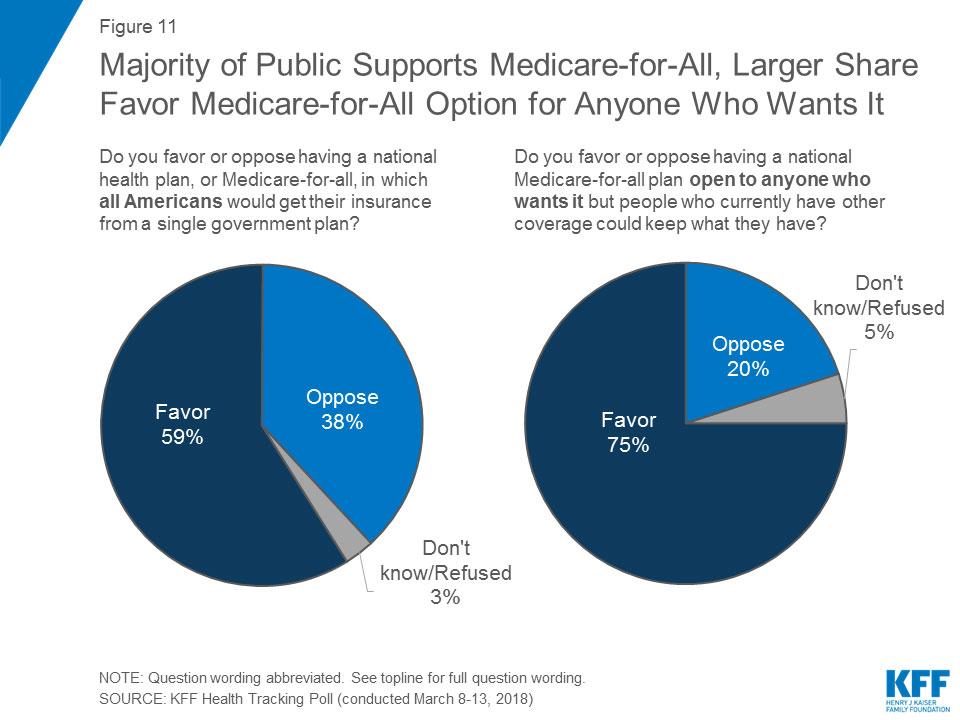
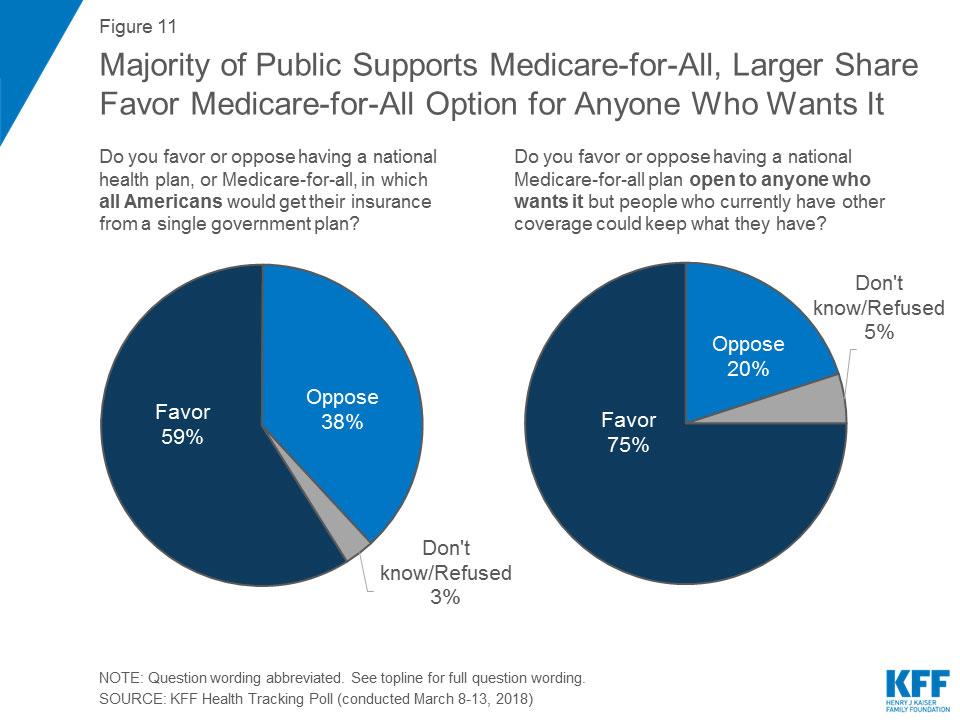
23/ This is from a national survey by the Kaiser Family Foundation (@KaiserFamFound), one of the most respected sources for this sort of data. They found that national Single Payer *is* popular…but guess what’s even MORE popular? That’s right: A robust Public Option.
24/ Most of the discussion on universal single payer has focused on financial issues: Taxes vs. savings, provider payments, etc. However, one other big issue which doesn’t get as much attention is whether it’s MANDATORY or not.
25/ A M4A proposal like Bernie’s (or Abdul’s, for Michigan) would make it MANDATORY for EVERYONE to switch over to it (in Bernie’s case, phased in over a 4 year period…not sure what the phase-in time for Abdul’s is).
26/ Here’s the thing: Nearly half the country (~155M people) are covered via Employer-based insurance. Some of it sucks, some is very good, most is in the middle. Every M4A/SP proposal promises that the new system would be much better (more comprehensive at a lower net cost)…
27/ …so on paper, you would THINK all 155M of those people would have no problem with this, right? Well, some might not, but human nature doesn’t work that way for the most part. People tend to cling to what they’re familiar with even if they’re not terribly happy with it.
28/ That means that in order to get people to accept a major change, especially something so personal as healthcare, you have to PROVE that it won’t just be a LITTLE better, it’ll be MUCH better. This is one area where I think SP advocates have painted themselves into a corner.
29/ Here’s what I mean: Just last week, a RIGHT-WING think tank came out with a big study which admitted that *total healthcare spending* in the U.S. would indeed save about $2 TRILLION over a decade under Bernie’s M4A proposal: acasignups.net/18/07/31/dear-…
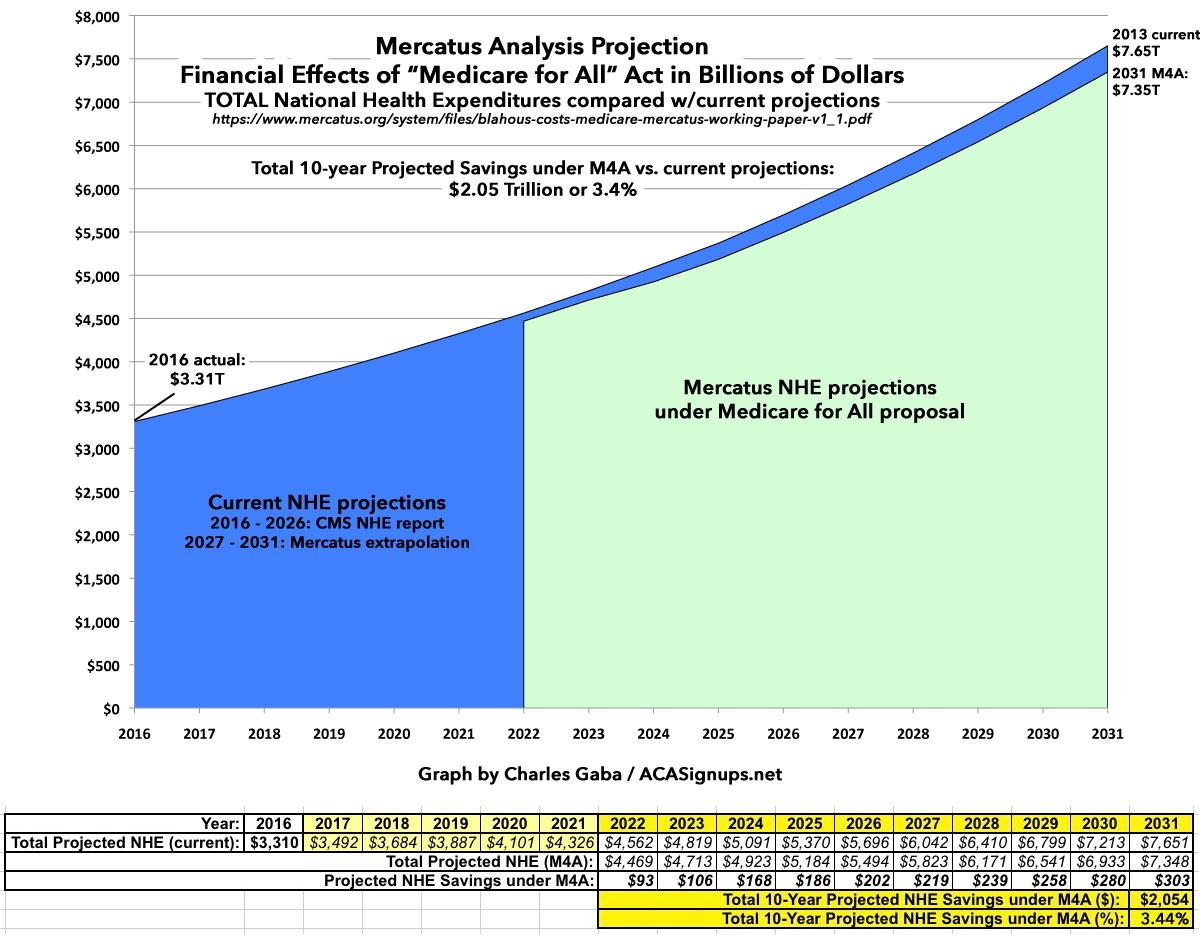
30/ That’s around a 3.5% savings. Bernie & Co. have been crowing about how this proves their point since even a right-wing wonk agrees M4A would save money. And *IF* he hadn’t spent the past 30 years insisting that moving to SP would cut healthcare costs in HALF, that’d be fine.
31/ Unfortunately, Bernie & Co keep pointing to charts like this which show “Every Other Industrialized Country” spending half as much or less on average. THAT’S the expectations bar they’ve set for M4A in the minds of most people. Suddenly, saving 3.5% seems far less impressive.

32/ Obviously the die-hard M4A/SP folks will dispute the 3.5% estimate as being too low, but you get my point:
33/ It’s not enough to say “what you have now is mediocre, I’m pretty sure what I have is somewhat better”.
You have to say “what you have now SUCKS, and I GUARANTEE what I have is FAR better.”
Even then, be prepared for a backlash from those who resent being forced to change.
You have to say “what you have now SUCKS, and I GUARANTEE what I have is FAR better.”
Even then, be prepared for a backlash from those who resent being forced to change.
34/ You know who learned this the hard way? President Obama, nearly 5 years ago.
As much as I admire him and as much as I support the ACA, his “If you like your plan you can keep it” promise was…um…poorly stated. Why? Because he forgot to include an important caveat.
As much as I admire him and as much as I support the ACA, his “If you like your plan you can keep it” promise was…um…poorly stated. Why? Because he forgot to include an important caveat.
35/ What he MEANT to say is that the people covered by their Employer, the VA, Medicare, Medicaid and CHIP wouldn’t have to worry about THEIR plans being replaced by a government plan, nor would anyone who enrolled in an Individual market plan before 2010.
36/ In other words, his “You Can Keep It” promise was about 98% accurate. The problem was the other 2%…perhaps 5-6 million people enrolled in Individual Market policies AFTER March 2010. Insurance carriers were given 4 years to transition those folks onto ACA-compliant plans.
37/ Most of the insurance carriers, of course, waited as long as they could to do this…namely, until they rolled out the 2014 plans in October 2013. Remember what happened next?
Those 5-6M people (I was among them) received cancellation notices from their insurance companies.
Those 5-6M people (I was among them) received cancellation notices from their insurance companies.
38/ Those 5-6M people were basically split into two groups: Some were in “junk plans” which were dirt cheap but really did suck ass. If you were on one of those AND qualified for ACA subsidies, you were probably fine with the change. Perhaps you grumbled a bit but got over it.
39/ Others, like myself, were enrolled in fairly GOOD plans. Not EVERY pre-ACA indy market plan sucked; some were pretty good. The problem is that even the good ones could still usually cherry-pick enrollees, throwing those w/pre-existing conditions under the bus.
40/ In my own case, my wife and I took it in stride—our pre-ACA decent plan was cancelled, so we replaced it with a post-ACA better plan. It cost more but also covered more, so we basically broke even. HOWEVER, many people screamed bloody murder.
41/ The backlash was so intense that Obama’s HHS Dept. was pressured into allowing the states to in turn allow the carriers to extend the deadline for their non-ACA plans by another year for existing enrollees. Then by ANOTHER year. Eventually it became effectively permanent.
42/ The point is, that backlash happened because a few million people were forced to switch policies after being promised they wouldn’t have to. Whether or not the new policy was better, the fact remains many of them “liked” their plans and resented being forced to drop it.
43/ Now extend that resentment to ~155 million people (OK, call it 100M if you assume 1/3 of those w/employer coverage hate it) and you see my larger point.
That’s why the question of making it MANDATORY vs. OPTIONAL is so important.
acasignups.net/18/03/27/whoa-…
That’s why the question of making it MANDATORY vs. OPTIONAL is so important.
acasignups.net/18/03/27/whoa-…
44/ OK, I’ll shut up for now, but I reserve the right to glom more onto this thread later. Meanwhile, I covered a lot of this and more in a snakier way in my one & only @Cracked article last year: cracked.com/blog/a-zero-b.…
• • •
Missing some Tweet in this thread? You can try to
force a refresh