
According to one neurosurgeon, my 2012 MRI (the self-same that my neurologist used to diagnose me with conversion disorder/hysteria) shows very clear signs of intracranial hypertension, most notably a pituitary gland that has been flattened into a pancake.
So when in #unrestfilm I say, "I can feel my brain pushing out my eyeballs" that is apparently true.
Of course I have been saying this for years, most notably when at the @GlendaleHosp ER last month, where I was diagnosed with "anxiety" and torticollis (tilting of the neck), even though the issue was that my neck COULD NOT TILT.
I said repeatedly I think I have too much pressure in my head, I need a lumbar puncture (less for diagnosis and more just to get some relief).
If I could wave a wand, I would make the following true:
1) This next generation of doctors would be taught zebras DO exist. If you can't diagnose your patient, the answer 9/10 is not that there is nothing wrong or that they're possessed by the usual convenient psychological spirits, but that you just haven't been able to figure it out
2) You can't possibly know everything and you shouldn't be expected to. But that also means your patient may know a lot more than you do. After all, they only have to specialize in one body and one clinical presentation.
So don't tell them what they are experiencing isn't happening. Instead, try to figure out *why.* The textbooks are not complete.
Lastly, and I know I've said this, but the ME/MCAD/EDS/POTS/Fibro/Lyme doctors and researchers really need to get together and figure out what is happening to all of us. They need to be trained to recognize potentially treatable co-morbidities.
This era of different diagnoses/research tracks/activist and philanthropic communities for patients with similar symptoms and similar treatments needs to end. We need radical collaboration and education.
We still obviously need dx-specific research, but when I rattle off to a Lyme doc my Rx's and he says, "Oh, those are the most commonly prescribed drugs in my practice." When an neurosurgeon says, "You look JUST like my post-viral EDS patients."
When orthostatic intolerance is in our #mecfs diagnostic criteria, but most patients aren't being properly evaluated for dysautonomia. When patients with the SAME onset, symptoms, presentation, response to treatment – in short, the same disease – are being given different labels.
When the ICC includes the hallmark symptoms of ME *and* hypermobility (#EDS?), food and fragrance intolerance (#MCAD?)...we aren't going to get clear on what is going on by simply sticking to our corners, trying to better define our boundaries.
We need boundaries, but I don't think we are truly going to be able to define them unless we take the dude with the ear, the woman with the tail, the guy with the snout, etc., and have an elephant-assembling party.
As someone who is the recipient of a huge volume of emails, I see patterns, connections and intriguing threads we MUST pull on. Internal heterogeneity is damaging to research. But so too is having people with the same conditions split across so many diagnoses.
And to anyone who is not a #spoonie reading at this hour, thanks for tuning in to what I'm sure is uninterpretable inside baseball. If you can, keep following and support us when you hear the call. Collectively, it's probably the fate of 100s of millions of people.
In case you're curious: a healthy person's MRI (right); my abnormal MRI and a pituitary pancake (left). Neurologists: do NOT believe a clean MRI report just because you get a clean MRI report. 
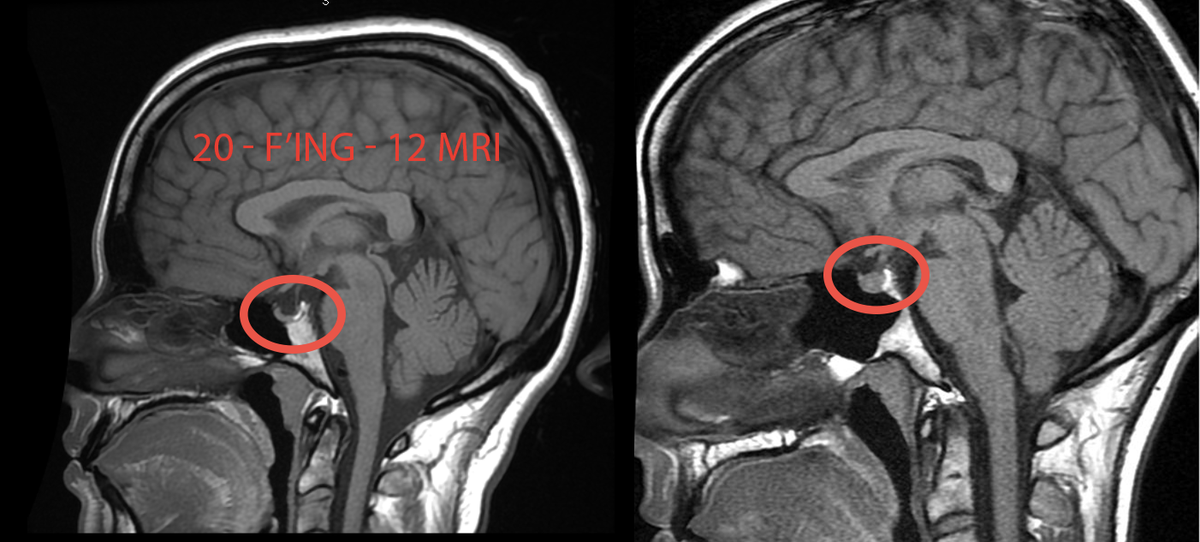
And please stop diagnosing patients whose symptoms you can't explain with conversion disorder (hysteria). Thanks.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



