Discover and read the best of Twitter Threads about #FiTSurvivalGuide
Most recents (24)

#FITSurvivalGuide: CV disease in Pregnancy #CardioObstetrics
#Tweetorial for new #CardiologyFIT by @MonSangh and @JennLewey @Penn
1⃣CV Physiology
2⃣Peripartum CM
3⃣SCAD
4⃣Valve Dz
5⃣Aortopathy
6⃣Arrhythmias
7⃣HTN Disorders of 🤰
8⃣🤰& Future CV Risk
9⃣Drug Safety
#Tweetorial for new #CardiologyFIT by @MonSangh and @JennLewey @Penn
1⃣CV Physiology
2⃣Peripartum CM
3⃣SCAD
4⃣Valve Dz
5⃣Aortopathy
6⃣Arrhythmias
7⃣HTN Disorders of 🤰
8⃣🤰& Future CV Risk
9⃣Drug Safety
1⃣CV Physiology
**Major changes occur to meet metabolic & circulatory needs of 🚼.
🔸Hemodynamic: ⬇️SVR/BP ⬆️HR/CO ⬆️Plasma ↔️Filling pressure
🔸Structural: ⬆️Chamber/LV mass ⬆️Aortic Compliance
🔸Cardiometabolic: ⬆️Insulin resistance ⬆️Lipid/Trig
**Major changes occur to meet metabolic & circulatory needs of 🚼.
🔸Hemodynamic: ⬇️SVR/BP ⬆️HR/CO ⬆️Plasma ↔️Filling pressure
🔸Structural: ⬆️Chamber/LV mass ⬆️Aortic Compliance
🔸Cardiometabolic: ⬆️Insulin resistance ⬆️Lipid/Trig


2⃣Peripartum Cardiomyopathy
🔸Epi: Blacks>>White
🔸Cause: Double-hit hypothesis
🔸Dx: Idiopathic, EF < 45%, ~ 1 m prior or 5 m after delivery
🔸Rx: HF tx; metoprolol/enalapril safe for lactation; ?bromocriptine, ?lactation
🔸LVEF recovery 👍 future risk
🔸Anticoagulation
🔸Epi: Blacks>>White
🔸Cause: Double-hit hypothesis
🔸Dx: Idiopathic, EF < 45%, ~ 1 m prior or 5 m after delivery
🔸Rx: HF tx; metoprolol/enalapril safe for lactation; ?bromocriptine, ?lactation
🔸LVEF recovery 👍 future risk
🔸Anticoagulation




Curious about how #POCUS is taught? This #Tweetorial is for U
#Preview for #ASEchoJC 🔜9/4 8pm EST
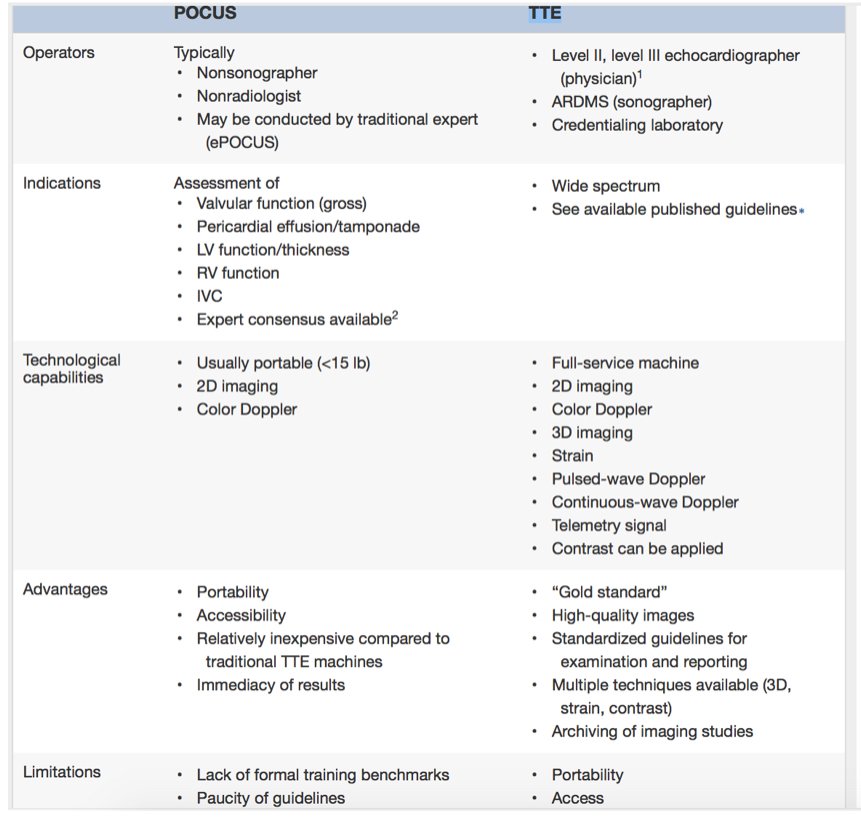
Point-of-Care Cardiac Ultrasound POCUS: State-of-the-Art in Medical School Education bit.ly/2wxD4PZ by @amerjohri
#POCUS not 🐇🎩, not short #TTE
#Preview for #ASEchoJC 🔜9/4 8pm EST
Point-of-Care Cardiac Ultrasound POCUS: State-of-the-Art in Medical School Education bit.ly/2wxD4PZ by @amerjohri
#POCUS not 🐇🎩, not short #TTE

2/ Current #goals #Cardiac #POCUS #MedEd
(1) introduce concepts of ultrasound- common imaging views, correlate with anatomy, & physical examination skills
(2) develop scanning techniques➡️ basic competence
(3) recognize & differentiate b/w normal anatomy & basic pathology
(1) introduce concepts of ultrasound- common imaging views, correlate with anatomy, & physical examination skills
(2) develop scanning techniques➡️ basic competence
(3) recognize & differentiate b/w normal anatomy & basic pathology


3/ When Do We Start? Prerequisite knowledge for #POCUS teaching
"priming effect" of preclinical education
Big machine 1st over handheld Martinez et al bit.ly/2wzCcJB @UMMC
Start 1st year @Hoppmann et al bit.ly/2Q4ECsO @UofSCSOM
"priming effect" of preclinical education
Big machine 1st over handheld Martinez et al bit.ly/2wzCcJB @UMMC
Start 1st year @Hoppmann et al bit.ly/2Q4ECsO @UofSCSOM

Another #FITSurvivalGuide tweetorial. This time on #intracoronary imaging w/ focus on IVUS and OCT
➡️ Rationale for use
➡️ Tech basics
➡️ Uses
➡️ Data
➡️ Images (high-yield)
➡️Comparison
@z_alirhayim @Almanfi_Cardio @AntoniousAttall @abashirMD @Babar_Basir
➡️ Rationale for use
➡️ Tech basics
➡️ Uses
➡️ Data
➡️ Images (high-yield)
➡️Comparison
@z_alirhayim @Almanfi_Cardio @AntoniousAttall @abashirMD @Babar_Basir
Why use them?
- Cor angio limited by: 2D view of 3D artery, diffuse dx, foreshortening, angulations, Ca++, eccentricity, vessel overlap, contrast streaming
- Angio alone ➡️ undetected edge complications, suboptimal stent exp in 15-20% ➡️ adverse events @cardiojaydoc02
- Cor angio limited by: 2D view of 3D artery, diffuse dx, foreshortening, angulations, Ca++, eccentricity, vessel overlap, contrast streaming
- Angio alone ➡️ undetected edge complications, suboptimal stent exp in 15-20% ➡️ adverse events @cardiojaydoc02
IVUS tech: US reflected from vessel wall
➡️ 2 types: Rotational; Phased-array
➡️Rotational: 40-45 MHz, 3.2 Fr, 5 Fr guide, Rx, better near field resolution
➡️Phased-array: 20 MHz, 3.5 Fr, 5 Fr guide, Rx, more trackable
➡️Co-registration with angio now available
➡️ 2 types: Rotational; Phased-array
➡️Rotational: 40-45 MHz, 3.2 Fr, 5 Fr guide, Rx, better near field resolution
➡️Phased-array: 20 MHz, 3.5 Fr, 5 Fr guide, Rx, more trackable
➡️Co-registration with angio now available



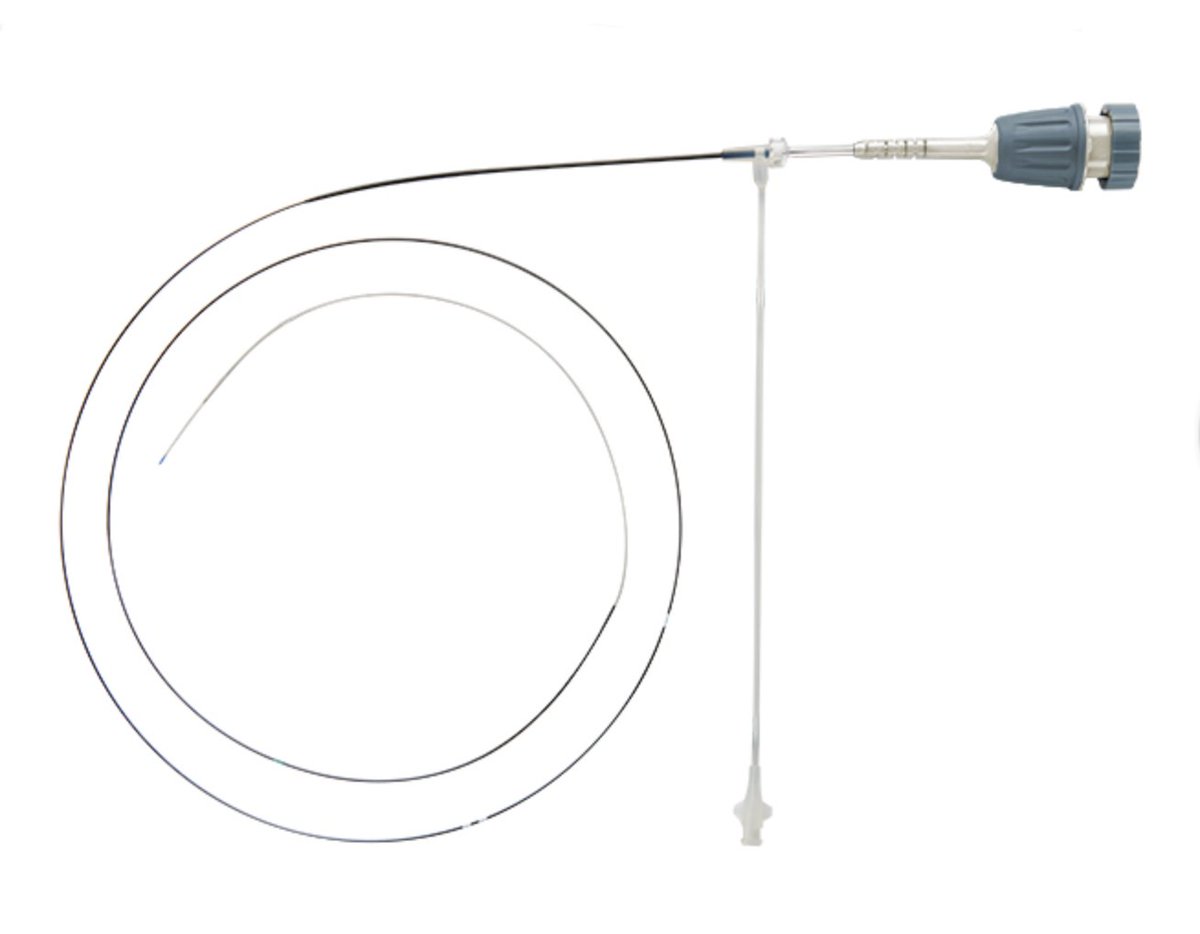
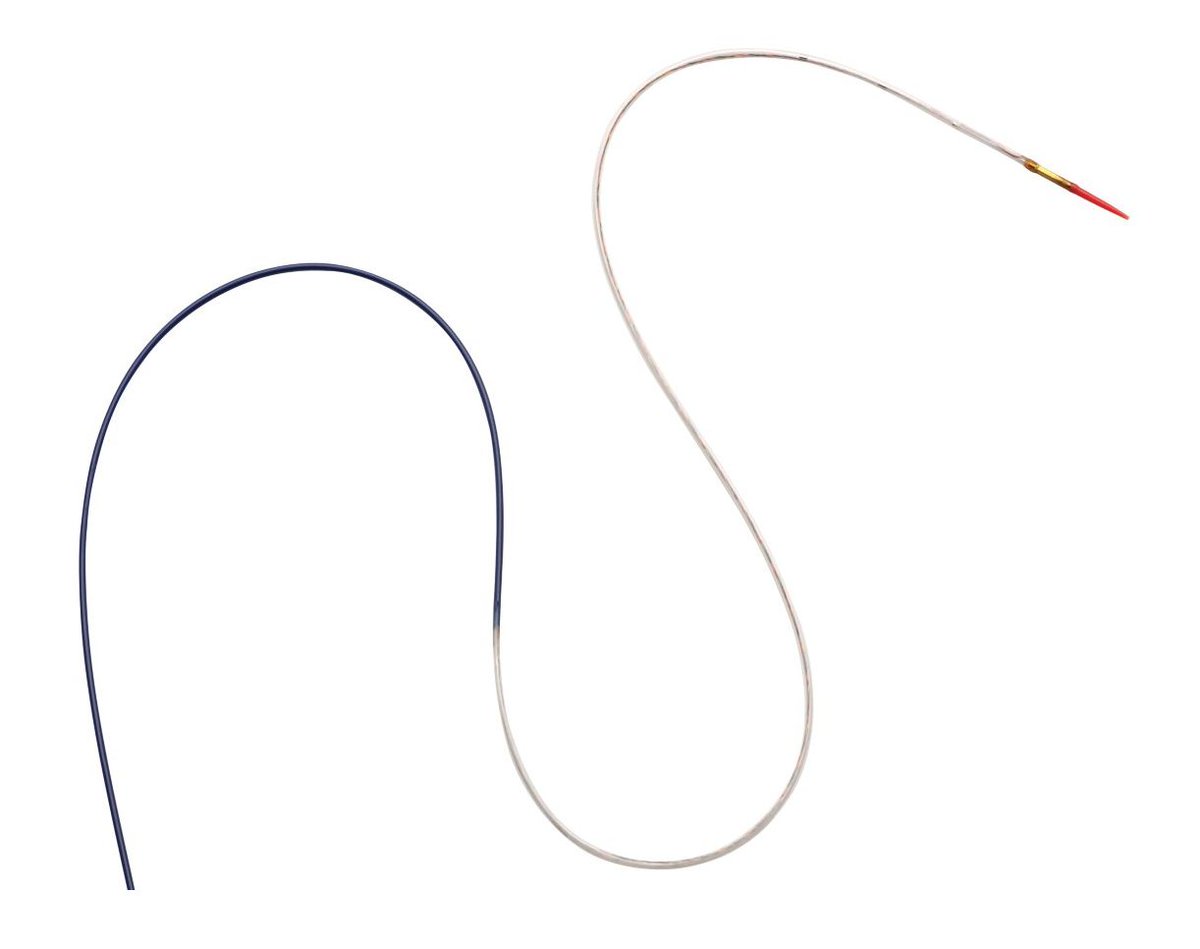
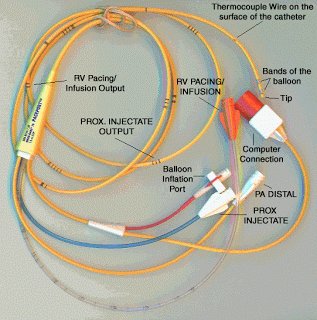
#FITSurvivalGuide - Right Heart Catheterizations
1⃣&2⃣ - Applications
3⃣ , 4⃣ , 5⃣ & 6⃣ - Data: Pressures, PCWP Waveform, CO & Shunts
7⃣ - Complications
Take home: RHC = useful diagnostic tool. Safe & effective use depends on thoughtful placement and data intepretation
1⃣&2⃣ - Applications
3⃣ , 4⃣ , 5⃣ & 6⃣ - Data: Pressures, PCWP Waveform, CO & Shunts
7⃣ - Complications
Take home: RHC = useful diagnostic tool. Safe & effective use depends on thoughtful placement and data intepretation
#FITSurvivalGuide - Right Heart Catheterizations
1⃣ - Applications
Accurate assessment of hemodynamics and etiology of shock
Assessment and management of severe HF e.g. "tailored therapy"
Evaluations of intracardiac shunts, valvular lesions
Perioperative management of severe HF
1⃣ - Applications
Accurate assessment of hemodynamics and etiology of shock
Assessment and management of severe HF e.g. "tailored therapy"
Evaluations of intracardiac shunts, valvular lesions
Perioperative management of severe HF
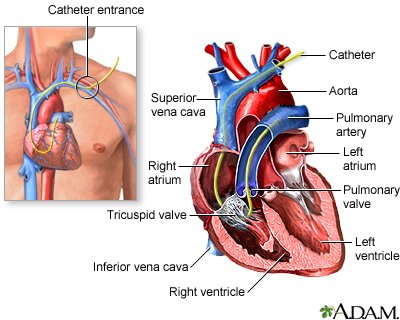
#FITSurvivalGuide - Right Heart Catheterizations
2⃣ - Applications
Risk stratification for patients considered for ❤️ Xplant
Establishing dx of PAH vs. secondary PH
Ddx: ❤️ vs non-❤️ cause of pulm edema (*caveat: RHC not indicated for routine mgmt of pulm edema or CHF)
2⃣ - Applications
Risk stratification for patients considered for ❤️ Xplant
Establishing dx of PAH vs. secondary PH
Ddx: ❤️ vs non-❤️ cause of pulm edema (*caveat: RHC not indicated for routine mgmt of pulm edema or CHF)

1/
As #ESCCongress nears, I thought I would do a #tweetorial on amyloidosis. Exciting times for the field and new data/treatments expected next week.
#FITSurvivalGuide #CardioTwitter @tony_breu @rodney_falk @marthagrogan1 @amyloidosisfdn @AmyloidosisSupp @Amyloidosis_ARC
As #ESCCongress nears, I thought I would do a #tweetorial on amyloidosis. Exciting times for the field and new data/treatments expected next week.
#FITSurvivalGuide #CardioTwitter @tony_breu @rodney_falk @marthagrogan1 @amyloidosisfdn @AmyloidosisSupp @Amyloidosis_ARC
2/
What is amyloidosis?
A protein misfolding disorder in which one of thirty-five distinct proteins pathologically misfolds and aggregates extracellularly as insoluble amyloid fibrils, ultimately leading to organ dysfunction.
What is amyloidosis?
A protein misfolding disorder in which one of thirty-five distinct proteins pathologically misfolds and aggregates extracellularly as insoluble amyloid fibrils, ultimately leading to organ dysfunction.

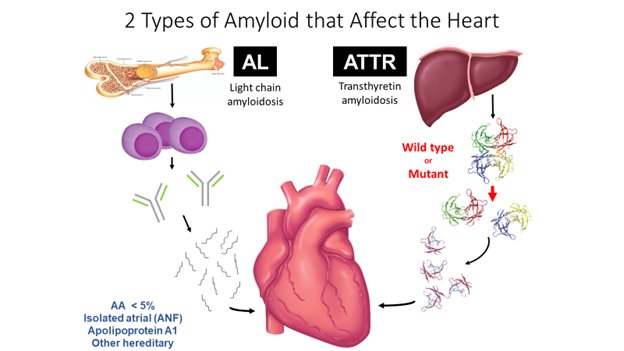
3/
You can see that other diseases like Alzheimer’s involve amyloid deposition. We will focus on two types of amyloidosis that affect the heart and nervous system: immunoglobulin light chain (AL) and transthyretin (ATTR) amyloidosis.
You can see that other diseases like Alzheimer’s involve amyloid deposition. We will focus on two types of amyloidosis that affect the heart and nervous system: immunoglobulin light chain (AL) and transthyretin (ATTR) amyloidosis.

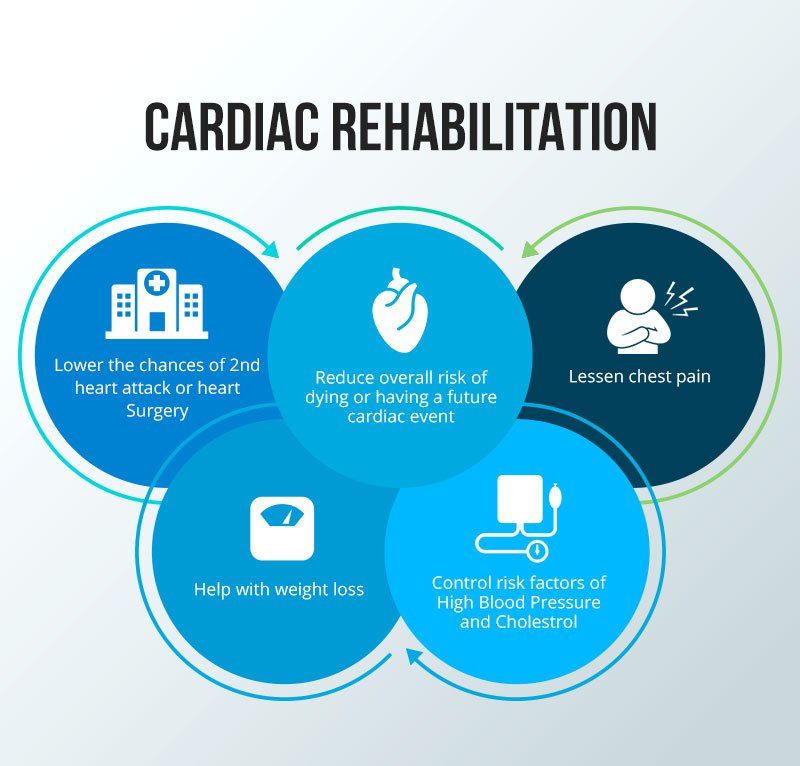
1/10 Cardiac Rehab – Secondary prevention #FITSurvivalGuide
1⃣Key Components
2⃣Benefits
3⃣Patients
4⃣Starting
5⃣Objective data
6⃣Patient limitations
7⃣Phase 1
8⃣Phase 2
9⃣Phase 3
1⃣Key Components
2⃣Benefits
3⃣Patients
4⃣Starting
5⃣Objective data
6⃣Patient limitations
7⃣Phase 1
8⃣Phase 2
9⃣Phase 3
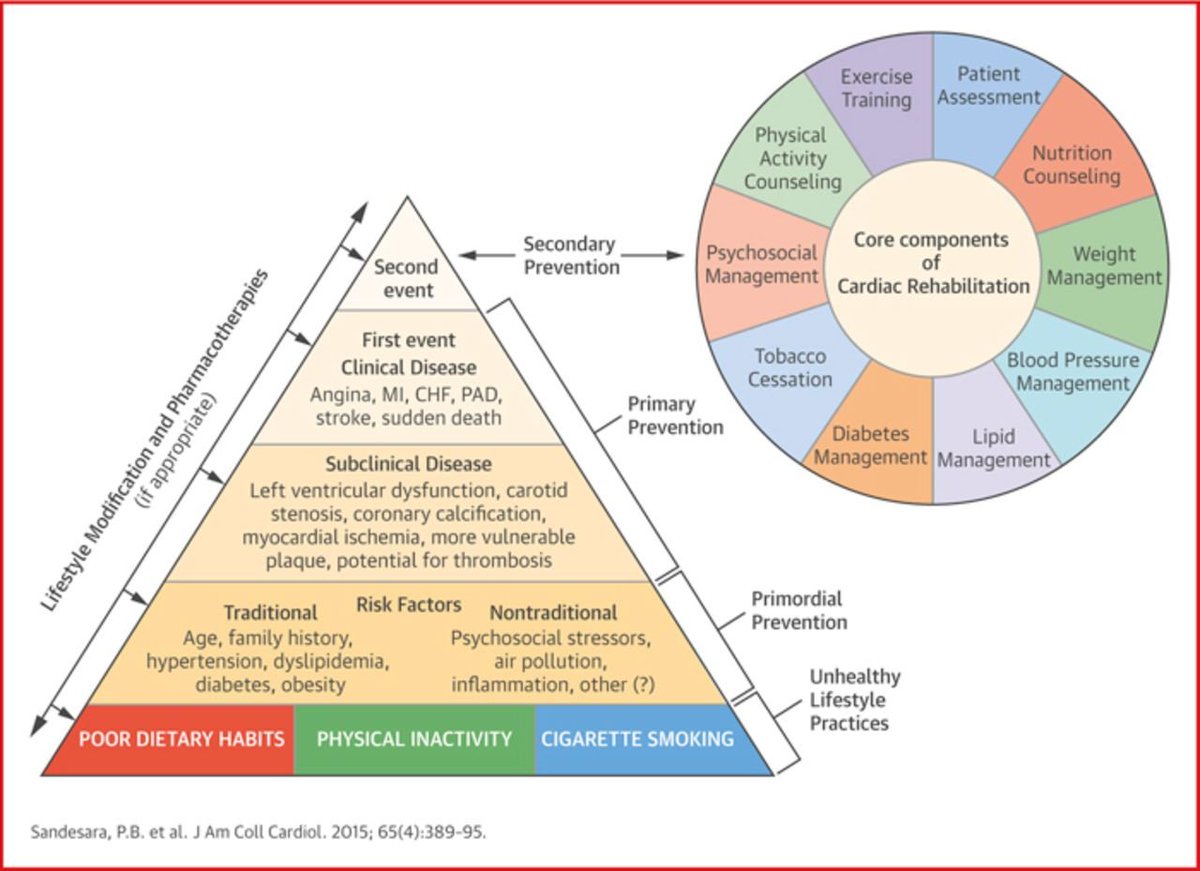
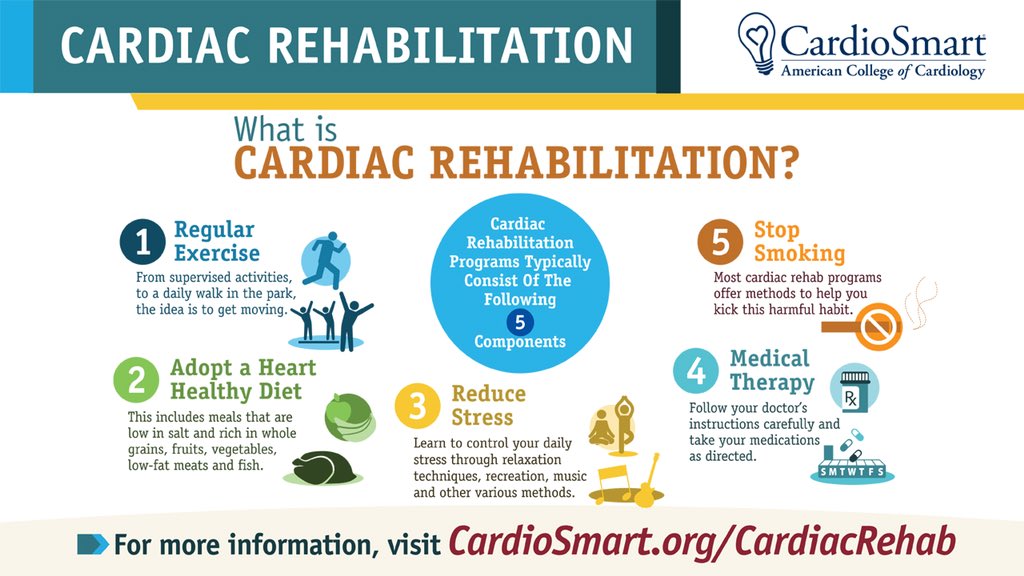
2/10 Cardiac Rehab – Secondary prevention #FITSurvivalGuide
1⃣Key Components
🚬 cessation, lipid mgmt, 🍄🍒🥥🥦🥬 counseling, ⬇️weight, 🆗blood pressure, psychosocial 🛋️, 🏋️♀️🏋️♂️⛹️♀️🏊♂️🏌️♀️🚣♂️⚽️, Diabetes mgmt
1⃣Key Components
🚬 cessation, lipid mgmt, 🍄🍒🥥🥦🥬 counseling, ⬇️weight, 🆗blood pressure, psychosocial 🛋️, 🏋️♀️🏋️♂️⛹️♀️🏊♂️🏌️♀️🚣♂️⚽️, Diabetes mgmt
3/10 Cardiac Rehab – Secondary prevention #FITSurvivalGuide
2⃣Benefits
Why? 25% mortality ⬇️, Benefit for >5yrs post-participation, ⬇️ symptoms, ⬇️ non-fatal MI for 1 year, ⬆️ 💊adherence, ⬆️ health factors, ⬇️ healthcare 💰💰.
2⃣Benefits
Why? 25% mortality ⬇️, Benefit for >5yrs post-participation, ⬇️ symptoms, ⬇️ non-fatal MI for 1 year, ⬆️ 💊adherence, ⬆️ health factors, ⬇️ healthcare 💰💰.

Evaluation of Cardiac Masses:
A Tweetorial for #FITSurvivalGuide 🚨 #ACCImaging @ASE360 @SCMR @journalofCMR @ACCinTouch
Dedicated:@dr_chirumamilla & all #ACCFIT in #CardioTwitter
Main Ref: link.springer.com/article/10.100… Palaskas, et al. Curr Treat Options Cardio Med (2018) 20: 29.
A Tweetorial for #FITSurvivalGuide 🚨 #ACCImaging @ASE360 @SCMR @journalofCMR @ACCinTouch
Dedicated:@dr_chirumamilla & all #ACCFIT in #CardioTwitter
Main Ref: link.springer.com/article/10.100… Palaskas, et al. Curr Treat Options Cardio Med (2018) 20: 29.

Usually, it all starts with an abnormal finding in an echo suggestive of intracavitary mass. How can we tell one from the other? It can be confusing.

For artifacts, I did a Tweetorial already that describes the most common ones. Basic understanding of ultrasound physics is needed to be able to explain them: twitter.com/i/moments/1030…

Our #FITSurvivalGuide continues with antiarrhythmic drugs! (AADs)
1️⃣Basic concepts
2️⃣Classification
3️⃣Class 1(a/b/c)
4️⃣Class 3
5️⃣Amio/dronedarone
6️⃣Clinical use
7️⃣Pearls and pitfalls
1️⃣Basic concepts
2️⃣Classification
3️⃣Class 1(a/b/c)
4️⃣Class 3
5️⃣Amio/dronedarone
6️⃣Clinical use
7️⃣Pearls and pitfalls

1️⃣ Arrhythmias originate from ectopy +/- reentry.
AADs work by:
*⬇️ing ectopy
*⬆️ing refractoriness (⬇️ing reentry)
AADs work by:
*⬇️ing ectopy
*⬆️ing refractoriness (⬇️ing reentry)
2️⃣
Class1: sodium channel blockers
(⬇️ ectopy, ⬇️ reentry by raising threshold for cell-cell conduction)
C2: beta blockers
C3: potassium channel blockers
(⬆️ action potential, ⬆️ AP "wavelength", ⬇️ excitable gap for reentry)
C4: calcium channel blockers
Class1: sodium channel blockers
(⬇️ ectopy, ⬇️ reentry by raising threshold for cell-cell conduction)
C2: beta blockers
C3: potassium channel blockers
(⬆️ action potential, ⬆️ AP "wavelength", ⬇️ excitable gap for reentry)
C4: calcium channel blockers

1/11
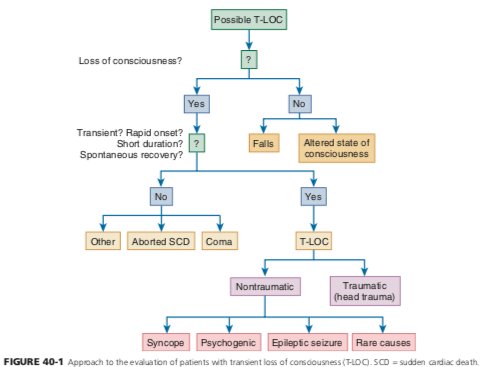
A #tweetorial on Syncope #FITsurvivalguide
Definition:
Sudden transient loss of consciousness with associated loss of postural tone, spontaneous recovery without neurologic deficits
The key is in the H&P
A good H&P can provide a dx in up to 50% of cases.
A #tweetorial on Syncope #FITsurvivalguide
Definition:
Sudden transient loss of consciousness with associated loss of postural tone, spontaneous recovery without neurologic deficits
The key is in the H&P
A good H&P can provide a dx in up to 50% of cases.

2
Goals.
1. Determine specific cause; this will direct therapy, prevent recurrences, ⬇️ expensive evaluations, and improve outcome.
2. Determine presence of cardiac syncope which portends ⬆️ mortality and sudden death.
3. Identify those who will benefit Inpt 🆚 outpt eval
Goals.
1. Determine specific cause; this will direct therapy, prevent recurrences, ⬇️ expensive evaluations, and improve outcome.
2. Determine presence of cardiac syncope which portends ⬆️ mortality and sudden death.
3. Identify those who will benefit Inpt 🆚 outpt eval
3/11
History
- Most important >> circumstance of syncope (ie. Prodrome), associated with particular activity? Exertion? change in position?
- Assess for sx of vasovagal syncope (most common cause)
- Duration of event
- Residual symptoms
History
- Most important >> circumstance of syncope (ie. Prodrome), associated with particular activity? Exertion? change in position?
- Assess for sx of vasovagal syncope (most common cause)
- Duration of event
- Residual symptoms






A #tweetorial on Perioperative risk assessment for Non-cardiac surgeries for #FITsurvivalguide
⚠️NOT "clearance"!
Purpose of consult
-Evaluate pt`s medical status
-Risk assessment
-Management recs
-Treat modifiable risk factors
-"Team" approach for shared decision making
⚠️NOT "clearance"!
Purpose of consult
-Evaluate pt`s medical status
-Risk assessment
-Management recs
-Treat modifiable risk factors
-"Team" approach for shared decision making
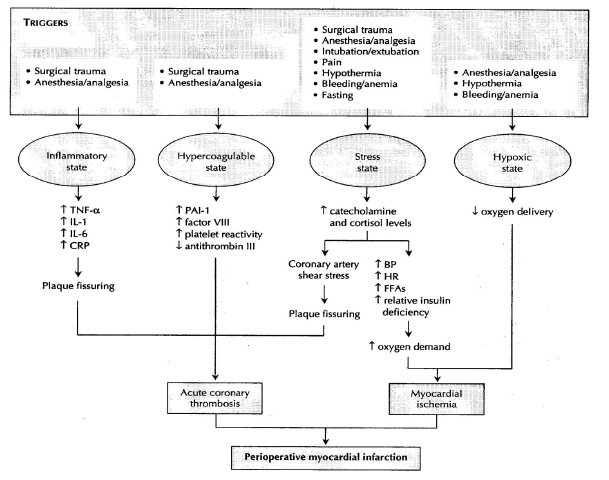
2/ Triggers for perioperative myocardial injury
-Inflammatory state
-Hypercoagulable state
-Stress state
-Hypoxic state
All predispose to ischemia and coronary thrombosis.
-Inflammatory state
-Hypercoagulable state
-Stress state
-Hypoxic state
All predispose to ischemia and coronary thrombosis.
3/ Think about- 🤔
-Should pt have surgery? Emergent or not?
-Type of surgery and type of anesthesia?
-Functional status of the pt?
-Relevant medical hx and any ongoing cardiac sx?
-Review the meds.
-Prior cardiac w/u.
Focus on good history and PE, can save a lot of tests & 💸
-Should pt have surgery? Emergent or not?
-Type of surgery and type of anesthesia?
-Functional status of the pt?
-Relevant medical hx and any ongoing cardiac sx?
-Review the meds.
-Prior cardiac w/u.
Focus on good history and PE, can save a lot of tests & 💸

#FITSurvivalGuide on Restrictive Cardiomyopathy (RCM) vs Constrictive Pericarditis (CP).
In both:
💠Diastolic RV & LV impaired; systolic function preserved
💠HFpEF phenotype, predominant “R sided” signs (JVP, edema, ascites)
1/12
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD
In both:
💠Diastolic RV & LV impaired; systolic function preserved
💠HFpEF phenotype, predominant “R sided” signs (JVP, edema, ascites)
1/12
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD
🔑 to understanding different filling:
RCM = myocardial disorder
CP = pericardial disorder.
2/12
@majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza @SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm @heartdoc45 @zainasadEP @docaward
RCM = myocardial disorder
CP = pericardial disorder.
2/12
@majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza @SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm @heartdoc45 @zainasadEP @docaward
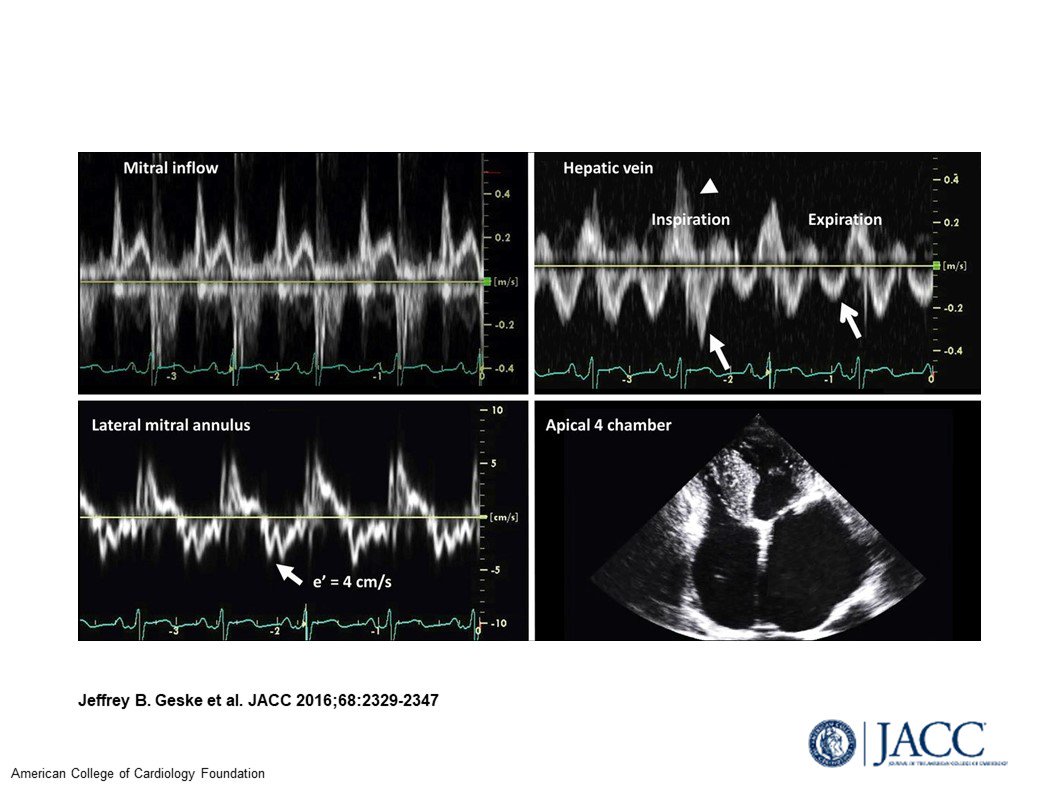
RCM
💠Stiff myocardium➡️early diastolic ⏫LV and RV pressure w/small vol ∆
💠 Echo: early diastolic abnormalities
💠High initial flow (= E wave; so E/A >2); ends abruptly (⬇️E decel time)
⚠️Restrictive pattern also in stage 3 HFrEF w/abnl early diastole
3/12
💠Stiff myocardium➡️early diastolic ⏫LV and RV pressure w/small vol ∆
💠 Echo: early diastolic abnormalities
💠High initial flow (= E wave; so E/A >2); ends abruptly (⬇️E decel time)
⚠️Restrictive pattern also in stage 3 HFrEF w/abnl early diastole
3/12

#FITSurvivalGuide: #HeartFailure management — a #tweetorial for #ACCFIT
1️⃣ Non-pharmacologic
2️⃣ Acute HF
3️⃣ Staging
4️⃣ HFrEF
5️⃣ HFpEF
6️⃣ Devices
7️⃣ Advanced Tx
8️⃣ Misc
Resources: @HFSA @ishlt @AHAScience @JACCJournals @HRSonline
1️⃣ Non-pharmacologic
2️⃣ Acute HF
3️⃣ Staging
4️⃣ HFrEF
5️⃣ HFpEF
6️⃣ Devices
7️⃣ Advanced Tx
8️⃣ Misc
Resources: @HFSA @ishlt @AHAScience @JACCJournals @HRSonline
1️⃣ Non-pharmacological therapies for HF:
➖Cardiac rehabilitation can improve functional capacity, exercise duration & mortality
➖Diet: Low Na (2-3 g/day) diet to reduce congestive symptoms
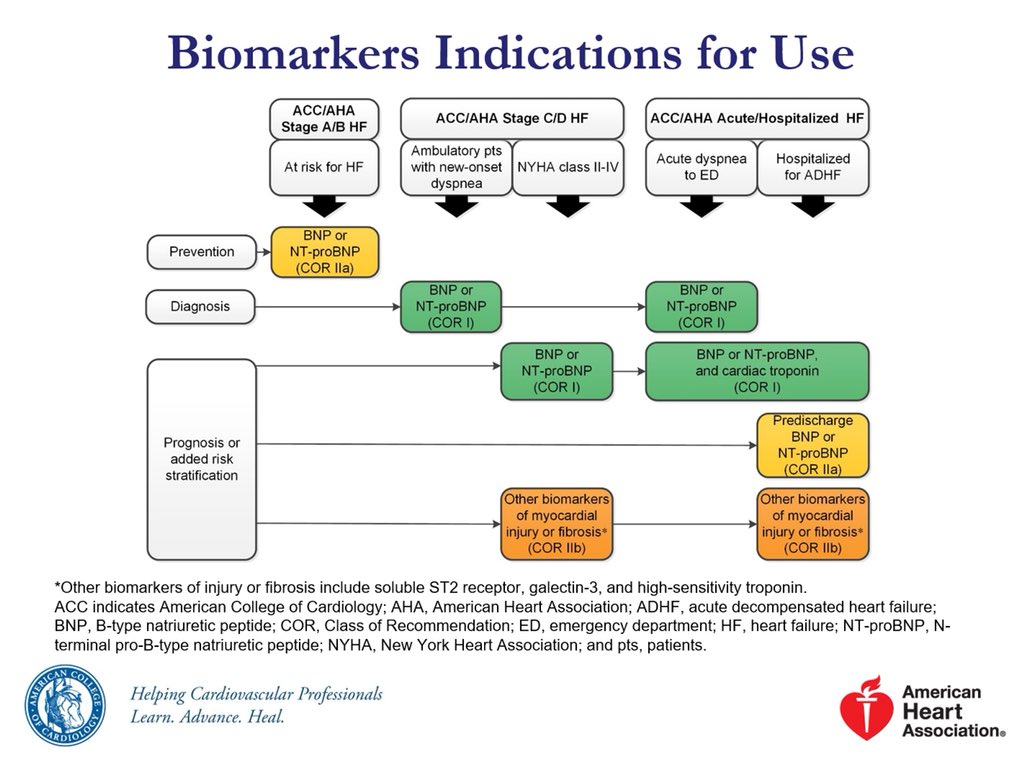
➖Biomarkers have an important role in diagnosis and prognosis of patients with HF
➖Cardiac rehabilitation can improve functional capacity, exercise duration & mortality
➖Diet: Low Na (2-3 g/day) diet to reduce congestive symptoms
➖Biomarkers have an important role in diagnosis and prognosis of patients with HF
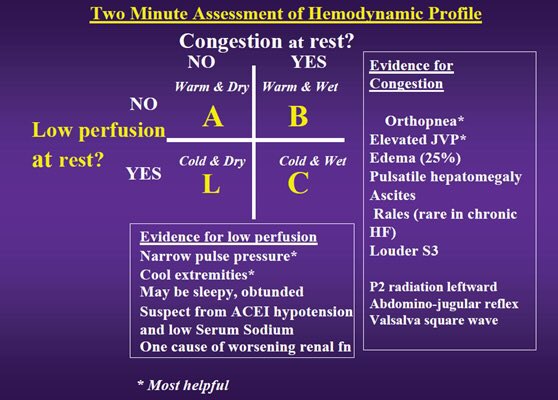
2️⃣ Acute Heart Failure Treatment agenda:
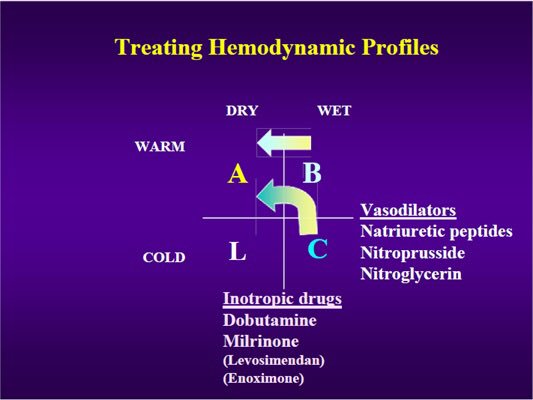
➖ Stabilize condition based on hemodynamics profile
➖ Establish dx, etiology and precipitating factor
➖ Initiate therapy for symptom relief
➖ Preload/afterload reduction
➖ Inhibition of neurohormonal activation for long term mgmt
➖ Stabilize condition based on hemodynamics profile
➖ Establish dx, etiology and precipitating factor
➖ Initiate therapy for symptom relief
➖ Preload/afterload reduction
➖ Inhibition of neurohormonal activation for long term mgmt

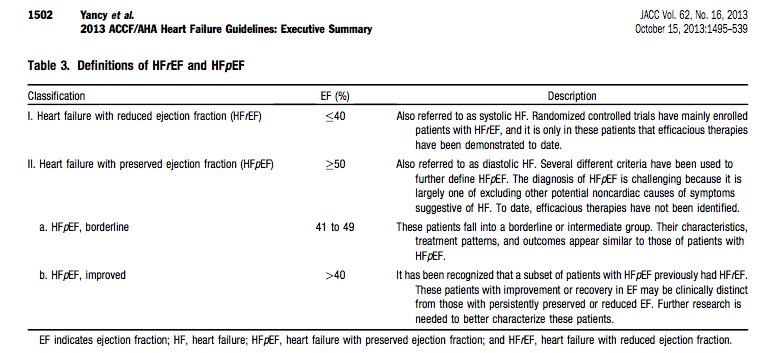
#FITSurvivalGuide #tweetorial Diagnosis of Heart failure: HF is a complex clinical syndrome related to structural or functional impairment of ventricular filling or contraction. HF can be classified into HFrEF and HFpEF based on assessment of LVEF.
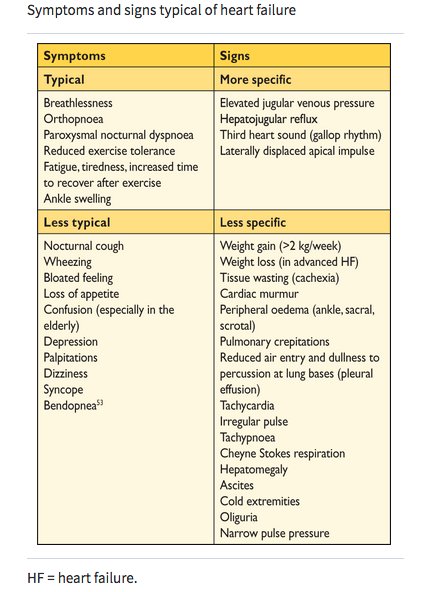
Typical HF symptoms are dyspnea, fatigue, edema, orthopnea, PND. NYHA system used to indicate symptom severity. Essential to inquire about onset, duration & progression of symptoms, risk factors for HF (MI, HTN, DM), FH of HF, drug or alcohol abuse, radiation/chemotherapy.

HF is a largely clinical diagnosis. Physical exam must include careful assessment of vital signs, signs of volume overload (JVD, edema, S3, rales on lung exam) and assessment of perfusion (cyanosis, cool extremities).

My #FITSurvivalGuide Tweetorial on the Dx/Rx of wide complex tachycardia: SVT vs VT
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD @majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @mmamas1973 @CMichaelGibson @DocSavageTJU @rajivxgulati @SVRaoMD @MinnowWalsh
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD @majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @mmamas1973 @CMichaelGibson @DocSavageTJU @rajivxgulati @SVRaoMD @MinnowWalsh
Step 1 w WCT is to assess ABCs. If the pt is unstable or in shock, it doesn't matter what the rhythm is> just shock the patient #FITSurvivalGuide
@sabeedak1 @noshreza @chadialraies @mirvatalasnag @venkmurthy @fischman_david i @vietheartPA @DrKevinCampbell @krishmd @cardiodee
@sabeedak1 @noshreza @chadialraies @mirvatalasnag @venkmurthy @fischman_david i @vietheartPA @DrKevinCampbell @krishmd @cardiodee
Step 2 for WCT is stop and think. Engage Kahneman's System 2 brain. Embrace Lord Bayes' concept of priors
What are the three reasons a tachy becomes wide?
#FITSurvivalGuide
@SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @heartdoc45 @zainasadEP @docaward @yogitar @KevinShahMD
What are the three reasons a tachy becomes wide?
#FITSurvivalGuide
@SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @heartdoc45 @zainasadEP @docaward @yogitar @KevinShahMD

#FITSurvivalGuide #ACCFIT
Topic - Ventricular Tachycardia!
Agenda:
1- Approach to evaluating #VT
2- Management of #VT
3- Practice Cases
Please share your thoughts & input to this #tweetorial!
@ACCCardioEd @ACCinTouch #FOAMed @MichiganACC
Topic - Ventricular Tachycardia!
Agenda:
1- Approach to evaluating #VT
2- Management of #VT
3- Practice Cases
Please share your thoughts & input to this #tweetorial!
@ACCCardioEd @ACCinTouch #FOAMed @MichiganACC
#FITSurvivalGuide #ACCFIT
1/10 – Ventricular Tachycardia
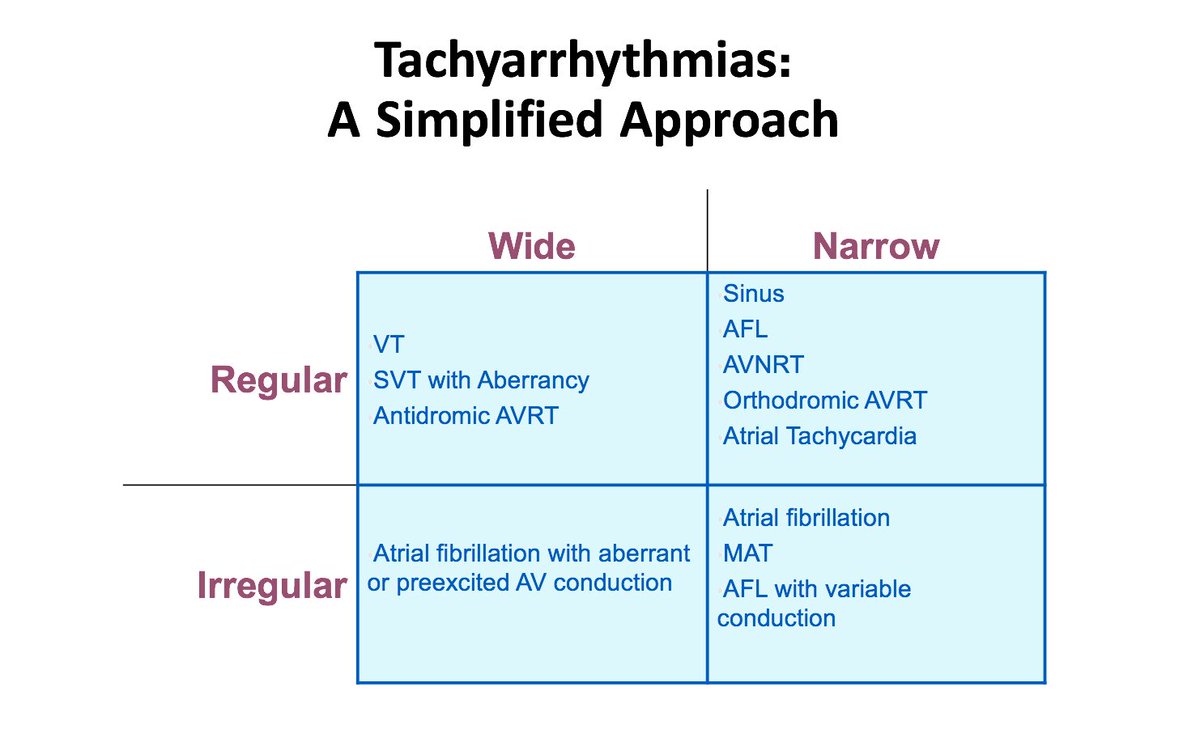
Simplified approach to evaluate tachycardia:
Rule #1 – If HD unstable ➡️ shock!
If HD stable, sit down & think.
Step # 1 - QRS: wide or narrow?
Step # 2 - Rhythm: regular or irregular?
This will narrow DDx!
1/10 – Ventricular Tachycardia
Simplified approach to evaluate tachycardia:
Rule #1 – If HD unstable ➡️ shock!
If HD stable, sit down & think.
Step # 1 - QRS: wide or narrow?
Step # 2 - Rhythm: regular or irregular?
This will narrow DDx!
#FITSurvivalGuide #ACCFIT
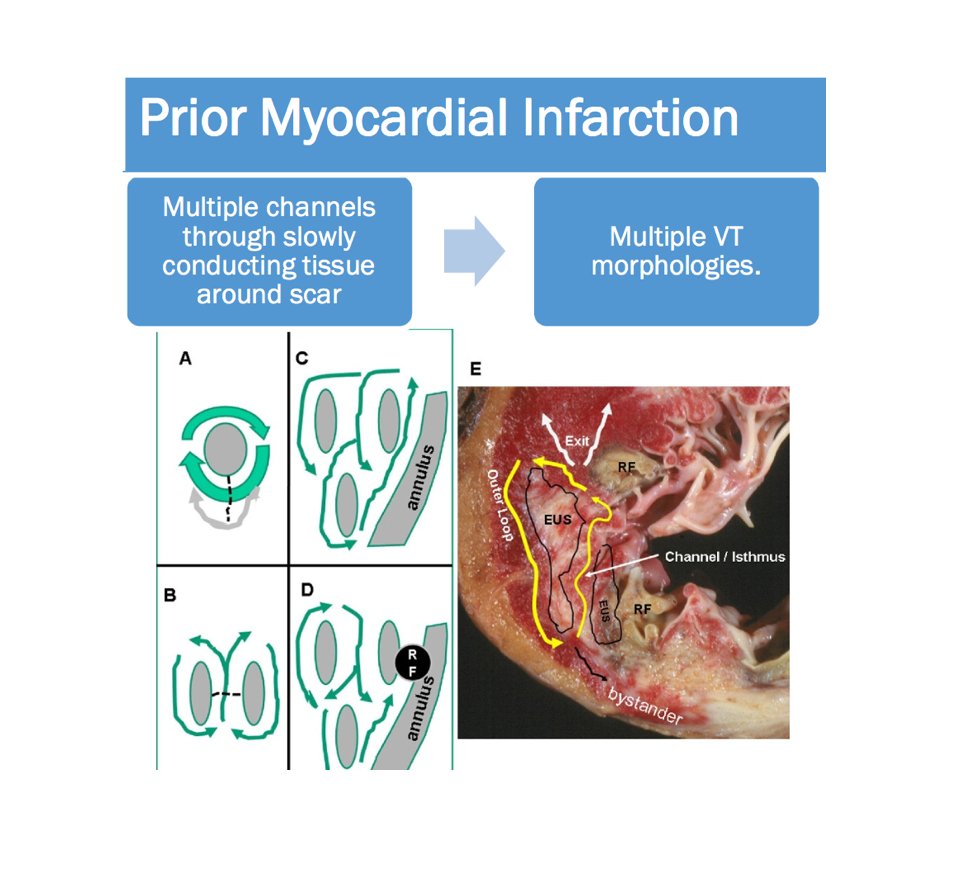
2/10 - Wide complex tachycardia
Always consider clinical Scenario!
Look for history of MI and cardiomyopathy ➡️ strongly favor #VT!
* If structural heart disease is present, you will be correct 9/10 times with diagnosis of VT!
2/10 - Wide complex tachycardia
Always consider clinical Scenario!
Look for history of MI and cardiomyopathy ➡️ strongly favor #VT!
* If structural heart disease is present, you will be correct 9/10 times with diagnosis of VT!

#FITSurvivalGuide #ACCFIT
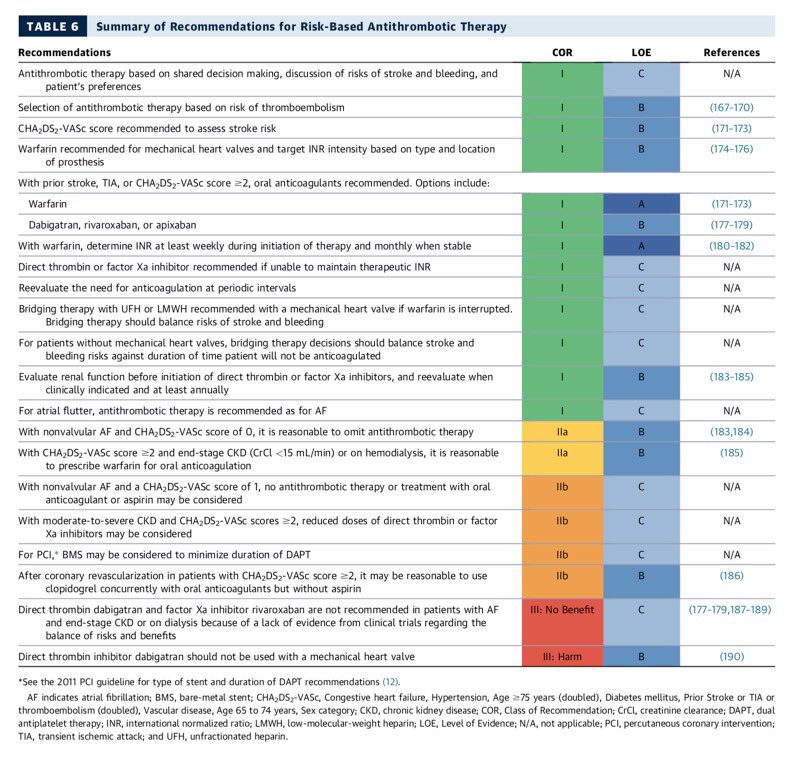
1/10: Stroke🧠 prevention in afib. #warfarin, #noacs, & LAA occlusion devices.
◽️shared decision making is key 🔑
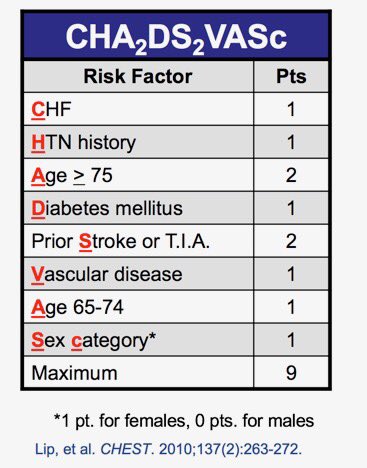
◽️CHADS-Vasc to stratify risk
◽️factor 💸and CrCl 🚽
◽️DAPT+AC= ↑↑bleeding
1/10: Stroke🧠 prevention in afib. #warfarin, #noacs, & LAA occlusion devices.
◽️shared decision making is key 🔑
◽️CHADS-Vasc to stratify risk
◽️factor 💸and CrCl 🚽
◽️DAPT+AC= ↑↑bleeding

2/10
For a quick review on coagulation physiology as it pertains to AC see 📽below.
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD @majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza
@SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm
For a quick review on coagulation physiology as it pertains to AC see 📽below.
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD @majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza
@SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm
3/10
Warfarin 🐀☣️
◽️interferes with normal post translational gamma-carboxylation of vitamin K dependent clotting factors 2️⃣7️⃣9️⃣🔟
◽️doesn’t inactivate functional clotting factors
◽️prothrombin half life: 72h
◽️Ergo INR effect 24-36 hr
🛑 teratogenic
Warfarin 🐀☣️
◽️interferes with normal post translational gamma-carboxylation of vitamin K dependent clotting factors 2️⃣7️⃣9️⃣🔟
◽️doesn’t inactivate functional clotting factors
◽️prothrombin half life: 72h
◽️Ergo INR effect 24-36 hr
🛑 teratogenic

#FITSurvivalGuide #ACCFIT
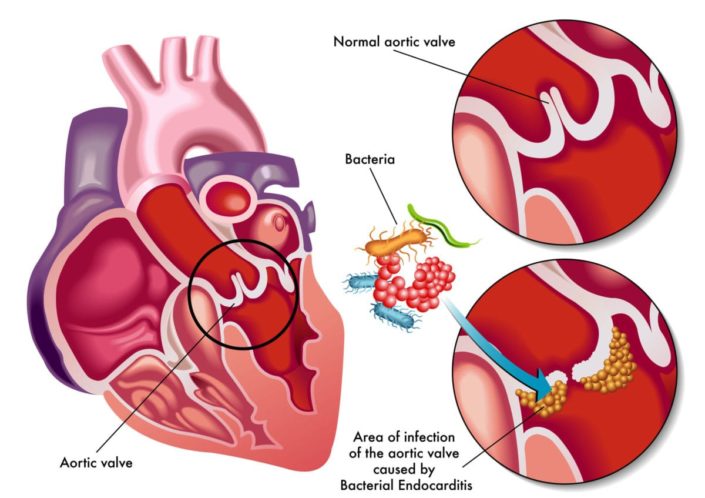
#InfectiveEndocarditis.
1/10 Not comprehensive. ⬇️⬇️some imp. points. Hx, exam, echo, micro data essential to diagnose & treat apporpriately. Suggested read : 2014 ACC/AHA valve guideline with 2017 Focused update.
cc: @dr_chirumamilla
#InfectiveEndocarditis.
1/10 Not comprehensive. ⬇️⬇️some imp. points. Hx, exam, echo, micro data essential to diagnose & treat apporpriately. Suggested read : 2014 ACC/AHA valve guideline with 2017 Focused update.
cc: @dr_chirumamilla
2/10
Incidence varies. Native IE 10-15/100K/year, PVE ~30% of all IE.
Risk ⬆️>60 years, ♂️sex, IV drug use, HIV, hemodialysis, poor 🦷 with infection, Alcoholic cirrhosis, intravascular device, CIED, immunosuppression, Transplants, Rheumatic ❤️ dz...
Incidence varies. Native IE 10-15/100K/year, PVE ~30% of all IE.
Risk ⬆️>60 years, ♂️sex, IV drug use, HIV, hemodialysis, poor 🦷 with infection, Alcoholic cirrhosis, intravascular device, CIED, immunosuppression, Transplants, Rheumatic ❤️ dz...


3/10
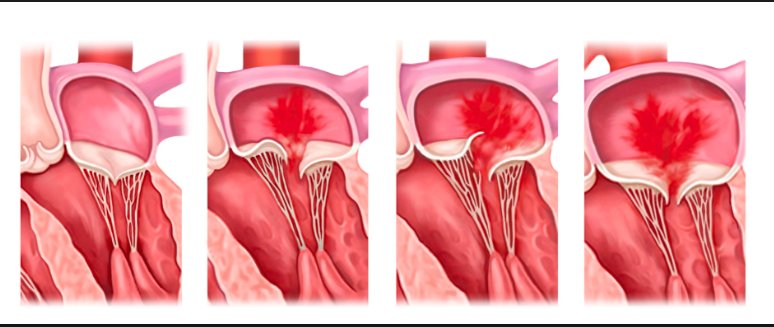
-Vegetations - "On the lower pressure side of a cardiac chamber / structural lesion or at site of impact of high-velocity blood jets "
-Acute vs Subacute IE
-Right vs Left sided IE
-Early (<60 days) vs Late ( >60days) Prosthetic IE
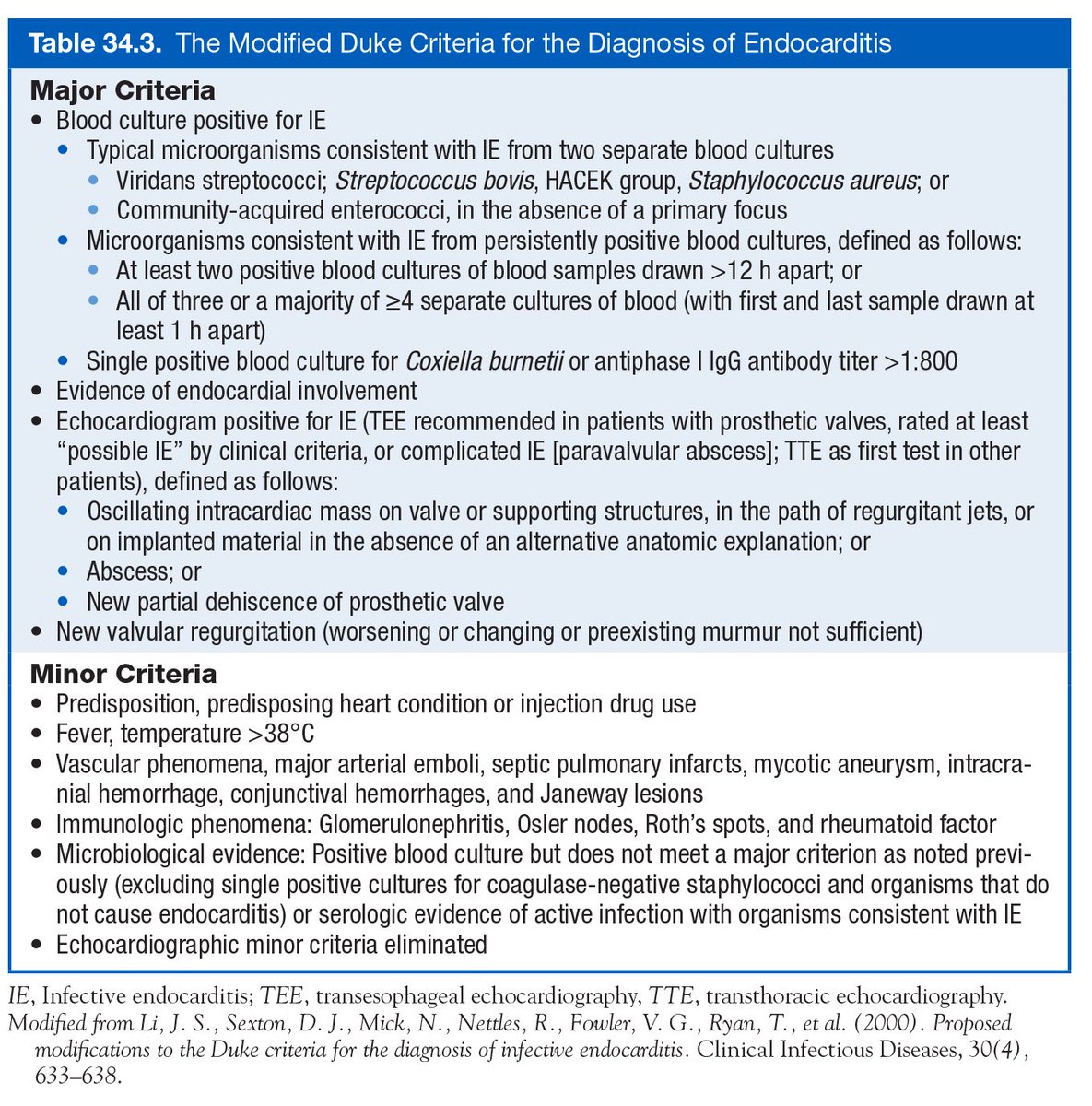
⭐️Modified Duke's criteria⭐️
-Vegetations - "On the lower pressure side of a cardiac chamber / structural lesion or at site of impact of high-velocity blood jets "
-Acute vs Subacute IE
-Right vs Left sided IE
-Early (<60 days) vs Late ( >60days) Prosthetic IE
⭐️Modified Duke's criteria⭐️




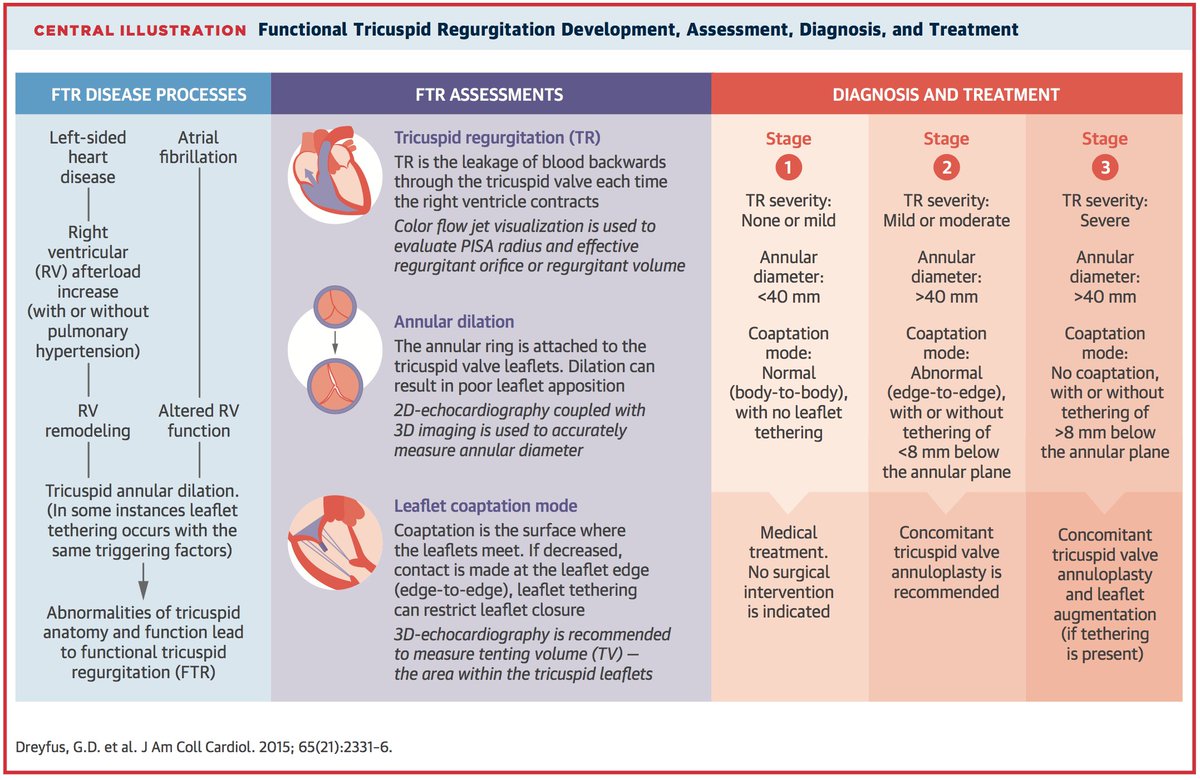
#FITSurvivalGuide: The Forgotten Valve-#TricuspidRegurgitation (#TR) #tweetorial for the new #ACCFIT!
1⃣ Anatomy
2⃣ Etiologies
3⃣ Classification
4⃣ Diagnosis
5⃣ Treatment
Resources: @ASE360 @JACCJournals @CircAHA @ACCCardioEd @UMNews @Medtronic
1/10
cc: @dr_chirumamilla
1⃣ Anatomy
2⃣ Etiologies
3⃣ Classification
4⃣ Diagnosis
5⃣ Treatment
Resources: @ASE360 @JACCJournals @CircAHA @ACCCardioEd @UMNews @Medtronic
1/10
cc: @dr_chirumamilla
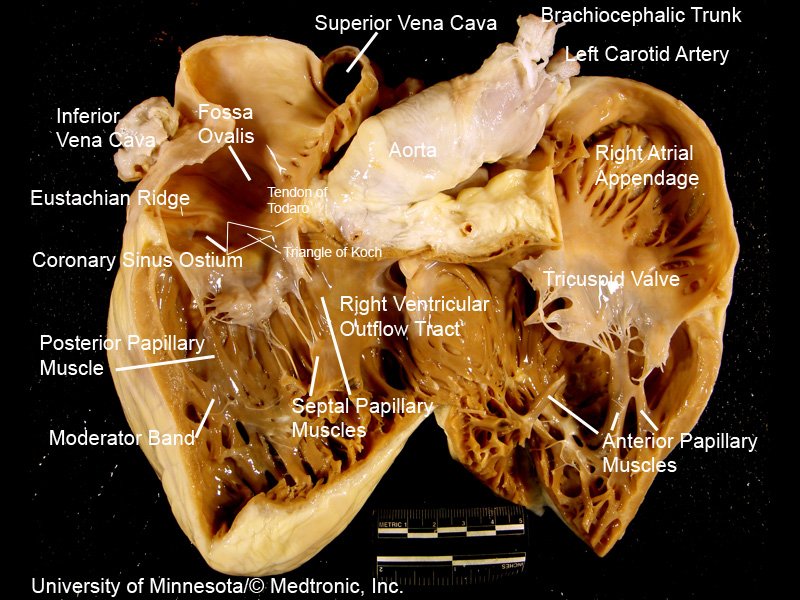
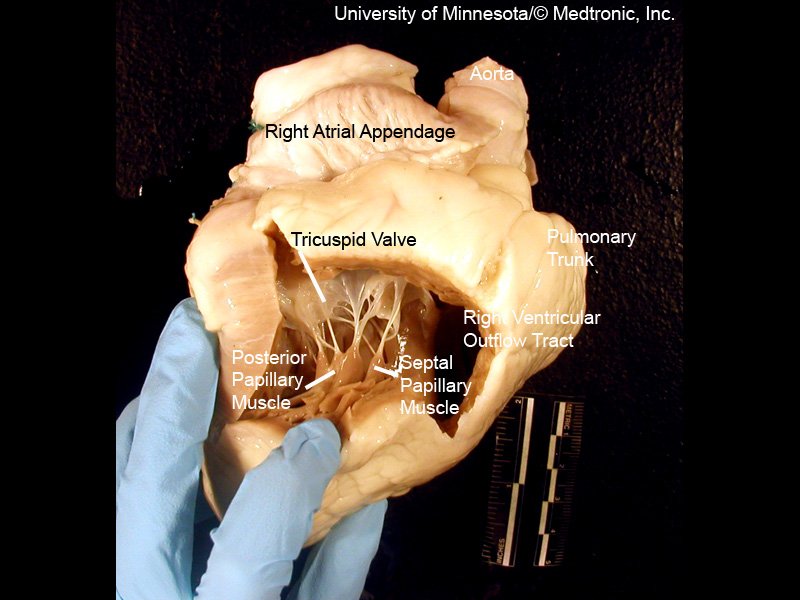
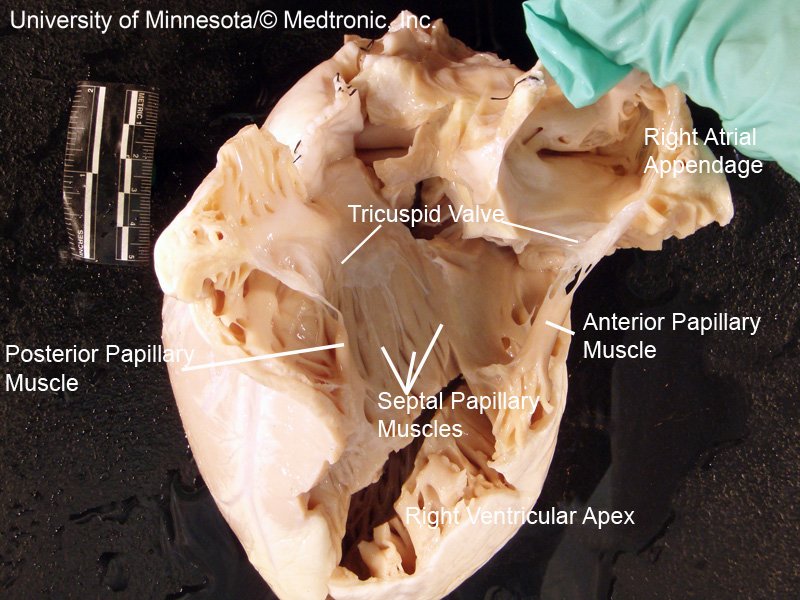
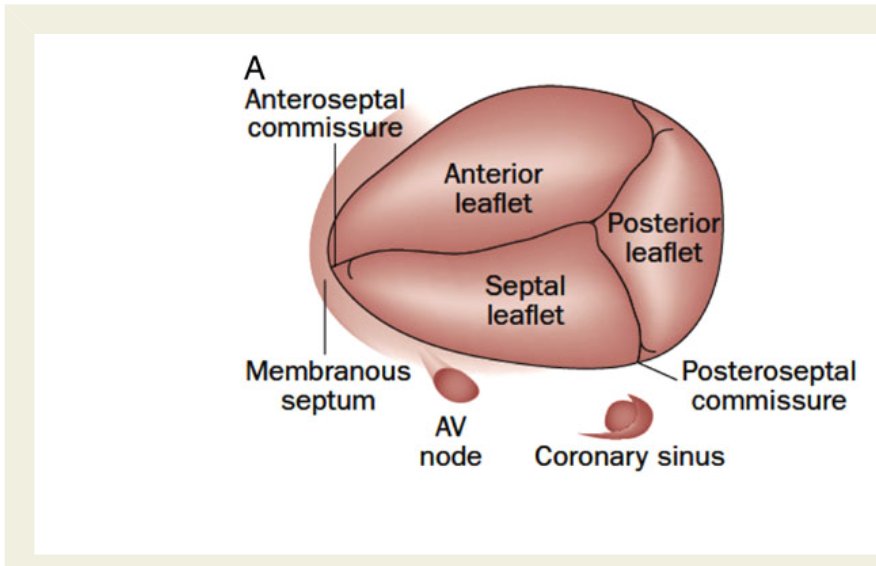
[2/10] Impt to understand #TricuspidValve 1⃣ Anatomy
3 leaflets ⬇️ + fibrous annulus + 2 papillary 💪🏽 + chordae tendinae + RA/RV ❤️
⬛️ Anterior 🍃 (largest)
◾️Posterior
▪️Septal (smallest)
(note: throughout #tweetorial, see image descriptions for more content)
3 leaflets ⬇️ + fibrous annulus + 2 papillary 💪🏽 + chordae tendinae + RA/RV ❤️
⬛️ Anterior 🍃 (largest)
◾️Posterior
▪️Septal (smallest)
(note: throughout #tweetorial, see image descriptions for more content)
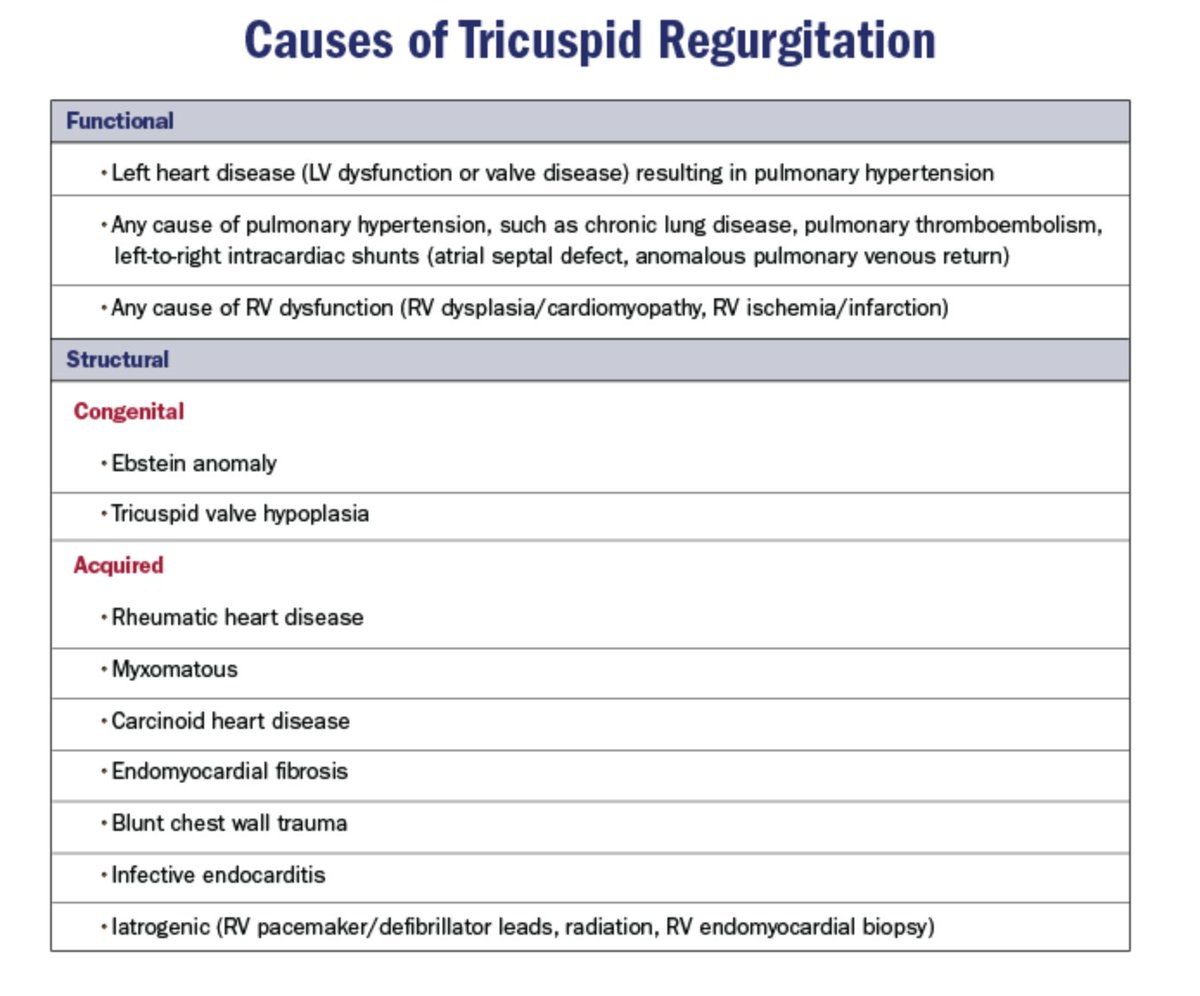
[3/10] 2⃣ Etiologies = Structural (1º) vs. Functional (FTR)
Keep chart ⬇️ DDx in mind when reading #EchoFirst
~80% of significant TR = FTR/2º to TA dilatation + leaflet tethering ⬅️ RV remodeling ⬅️ volume and/or pressure overload
Structural (1º) cause = less common
Keep chart ⬇️ DDx in mind when reading #EchoFirst
~80% of significant TR = FTR/2º to TA dilatation + leaflet tethering ⬅️ RV remodeling ⬅️ volume and/or pressure overload
Structural (1º) cause = less common

Continuing #FITSurvivalGuide: Brief outlook Mitral Regurgitation (MR) Management
(awesome part 1 of MR dx by @sairasamani)
⬆️age = ⬆️incident MR requiring ?🏥zations/intervention -->healthcare 💰💰
Untreated severe MR ass. w/ poor outcomes 2/2 volume overload of the ❤️
(awesome part 1 of MR dx by @sairasamani)
⬆️age = ⬆️incident MR requiring ?🏥zations/intervention -->healthcare 💰💰
Untreated severe MR ass. w/ poor outcomes 2/2 volume overload of the ❤️
2⃣/ First Step: Primary Vs Secondary MR? 🧐
Secondary MR --> further to be classified as ischemic or non ischemic in origin.
Identify MR Etiology by Carpentier Functional Classification
(see image: El Sabbagh, A. et al. J Am Coll Cardiol Img. 2018;11(4):628–4)
Secondary MR --> further to be classified as ischemic or non ischemic in origin.
Identify MR Etiology by Carpentier Functional Classification
(see image: El Sabbagh, A. et al. J Am Coll Cardiol Img. 2018;11(4):628–4)
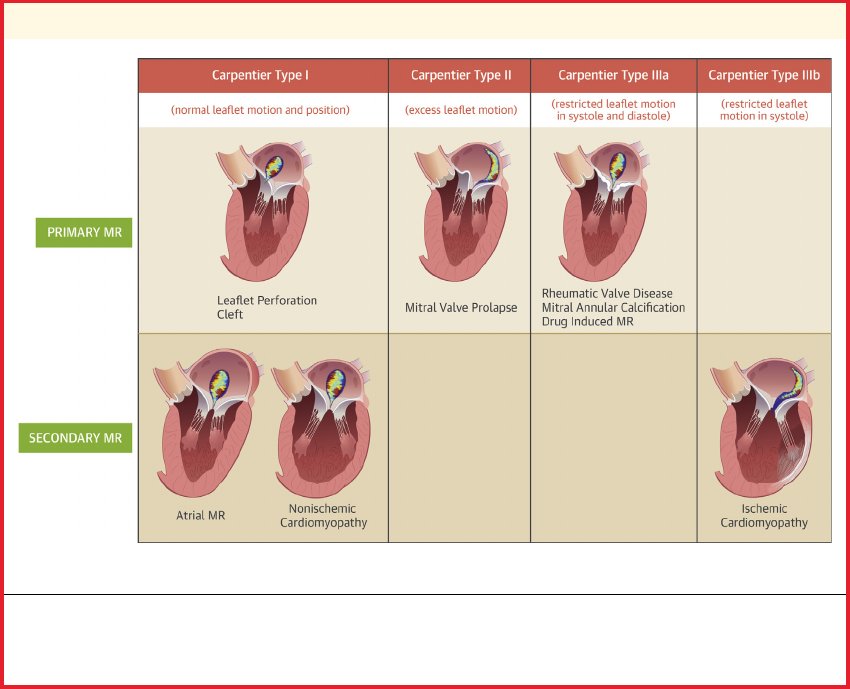
3⃣/ Primary MR:
Asymptomatic patients w/ severe primary MR preserved LVEF(>60%, LV end-sys dimension <40 mm [stage C1]) ▶️ mitral valve surgery is reasonable in the setting of serial imaging studies that reveal a progressive increase in LV size or decrease in LVEF (Class IIa)
Asymptomatic patients w/ severe primary MR preserved LVEF(>60%, LV end-sys dimension <40 mm [stage C1]) ▶️ mitral valve surgery is reasonable in the setting of serial imaging studies that reveal a progressive increase in LV size or decrease in LVEF (Class IIa)


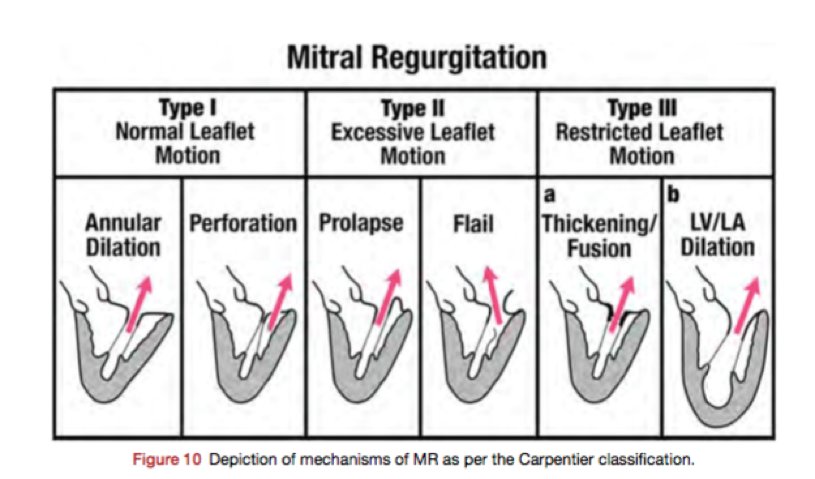
#FITSurvivalGuide 1/10 Tweetorial on MR. From JASE April 2017. This is an extensive topic, and a tweetorial will not do justice, so highly recommend to read this article. @ASE360 @ACCCardioEd @newmexicoacc #echoboards

2/10
MR can be 1’ or 2’. Simplified version: 1’ MR d/t pathology of the valve itself. 2’ MR = MV apparatus is intact, w/ ventricular disease (LV dilatation) dilated MV annulus to MV leaflets malcoaptation MR (~central jet). Also useful to use Carpentier classification.
MR can be 1’ or 2’. Simplified version: 1’ MR d/t pathology of the valve itself. 2’ MR = MV apparatus is intact, w/ ventricular disease (LV dilatation) dilated MV annulus to MV leaflets malcoaptation MR (~central jet). Also useful to use Carpentier classification.
3/10
Determine the scallops. First heard from @MayoClinicCV: 2 steps
1.At 0 deg: Determine if ant or post leaflet abn
2.At 60 deg: Determine which scallop 1,2, or 3
Pic from J Am Soc Echocardiogr 2013;26:921-64
Determine the scallops. First heard from @MayoClinicCV: 2 steps
1.At 0 deg: Determine if ant or post leaflet abn
2.At 60 deg: Determine which scallop 1,2, or 3
Pic from J Am Soc Echocardiogr 2013;26:921-64


1/10 What is chest pain? #FITSurvivalGuide #Tweetorial
- "Pain anywhere in the chest" 🤦♀️
- Many things cause chest pain
- ❤️ vs ❌❤️
- ❤️ - ischemic vs non ischemic
- Life threatening vs not
- "Pain anywhere in the chest" 🤦♀️
- Many things cause chest pain
- ❤️ vs ❌❤️
- ❤️ - ischemic vs non ischemic
- Life threatening vs not
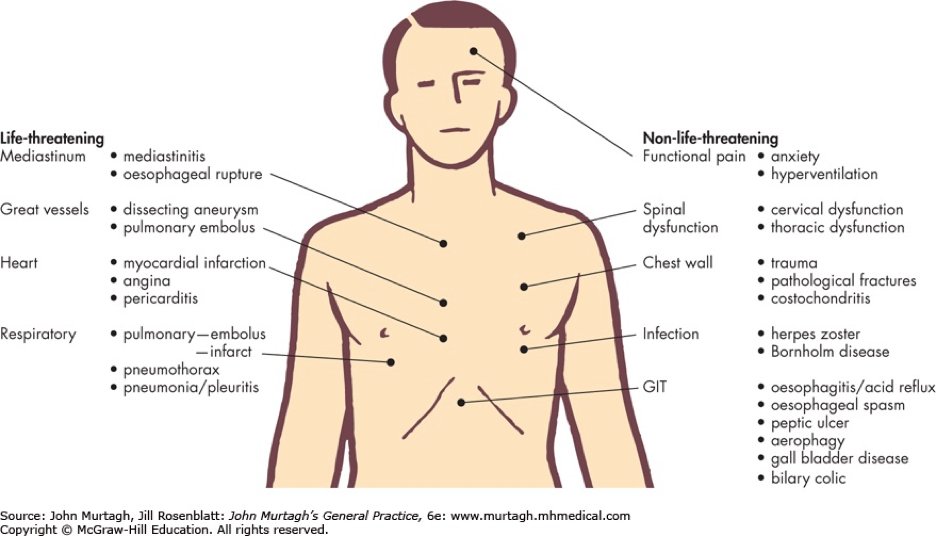
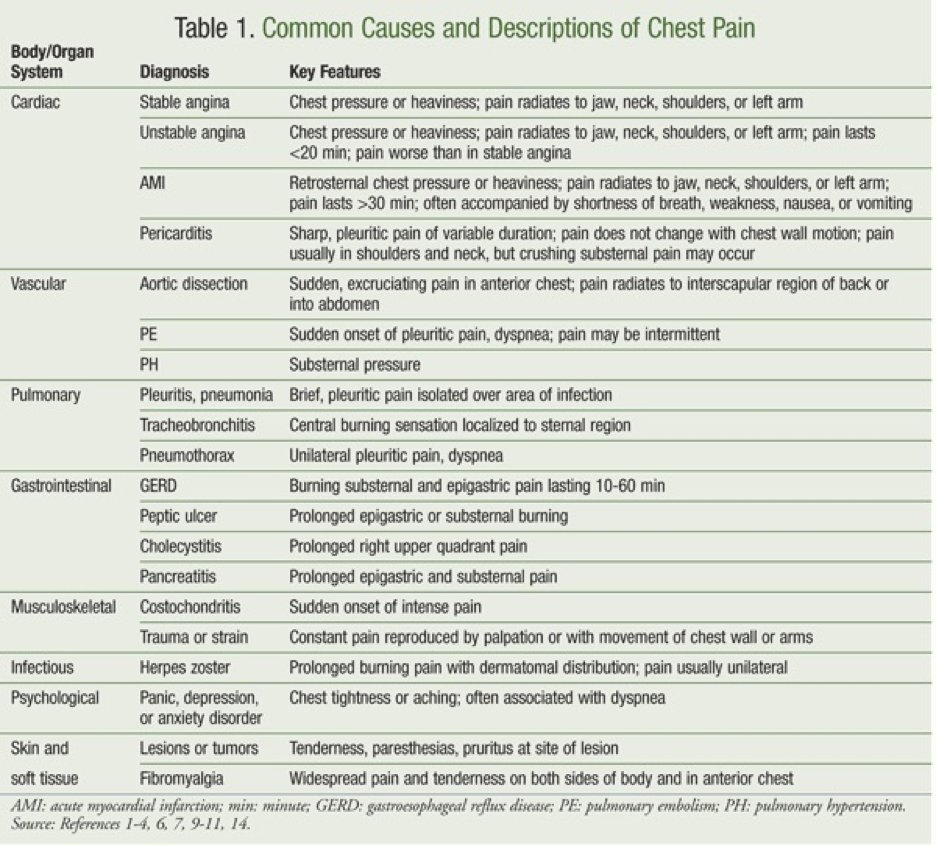
2/10 - Common causes of chest pain (by system) #FITSurvivalGuide
- Cardiac
- Pulmonary
- GI
- MSK
- Infectious
- Psych
- Skin/ soft tissue
- Cardiac
- Pulmonary
- GI
- MSK
- Infectious
- Psych
- Skin/ soft tissue
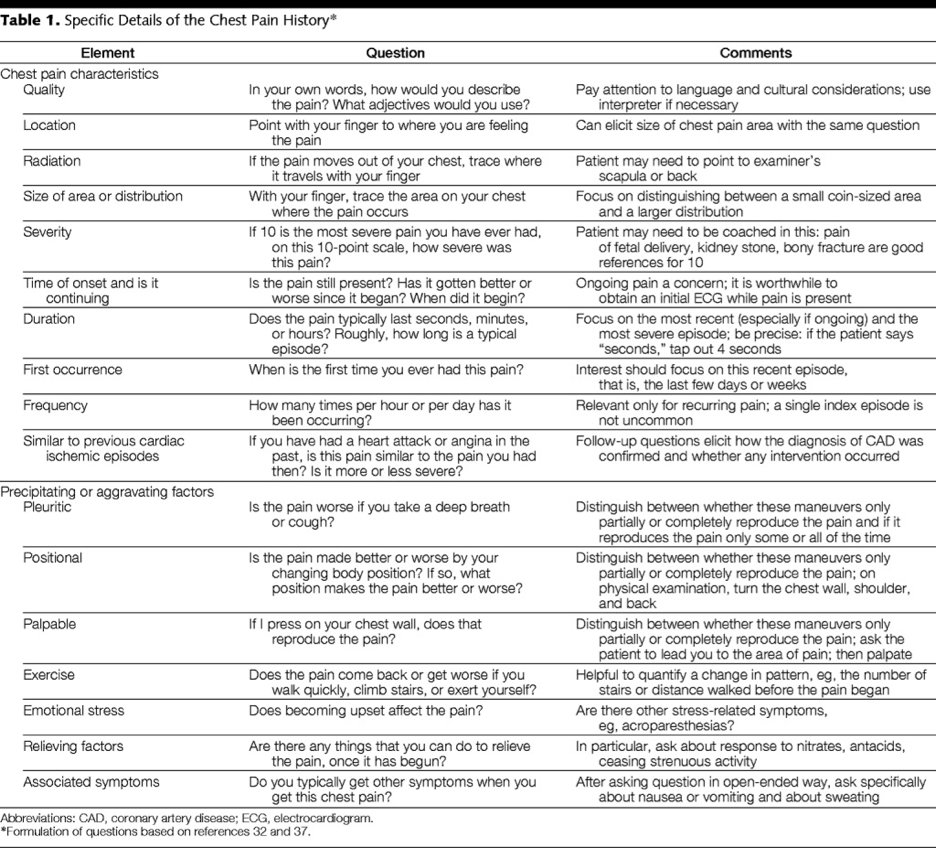
3/10 Chest pain- The History! #FITSurvivalGuide
- Going back to medical school 👩⚕️👨⚕️🥼😷
- The key to figuring out what type of chest pain the patient has!
- Quality, location, radiation, duration, associated symptoms, relieving factors!
- Going back to medical school 👩⚕️👨⚕️🥼😷
- The key to figuring out what type of chest pain the patient has!
- Quality, location, radiation, duration, associated symptoms, relieving factors!

#FITSurvivalGuide Aortic Emergency style!
Will discuss presentation/dx/complications/tx for:
1. Aortic dissection💉
2. IMH❣️
3. PAU
4. Traumatic transection
5. Non-emergent aneurysm surgical cutoffs (because boards loves them!)
Hoping @keaglemd can share his expertise as well!
Will discuss presentation/dx/complications/tx for:
1. Aortic dissection💉
2. IMH❣️
3. PAU
4. Traumatic transection
5. Non-emergent aneurysm surgical cutoffs (because boards loves them!)
Hoping @keaglemd can share his expertise as well!
Everyone please feel free to add to this thread for more learning #FIT #CardioEd
@dr_chirumamilla @APostalian @heartdoc45 @Babar_Basir @DrJayMohan @SamRRazaMD @DocStrom @DocSavageTJU @SamRRazaMD @DrQuinnCapers4 @cardiojaydoc02 @DrSheilaSahni @saraceciliamtz @onco_cardiology
@dr_chirumamilla @APostalian @heartdoc45 @Babar_Basir @DrJayMohan @SamRRazaMD @DocStrom @DocSavageTJU @SamRRazaMD @DrQuinnCapers4 @cardiojaydoc02 @DrSheilaSahni @saraceciliamtz @onco_cardiology
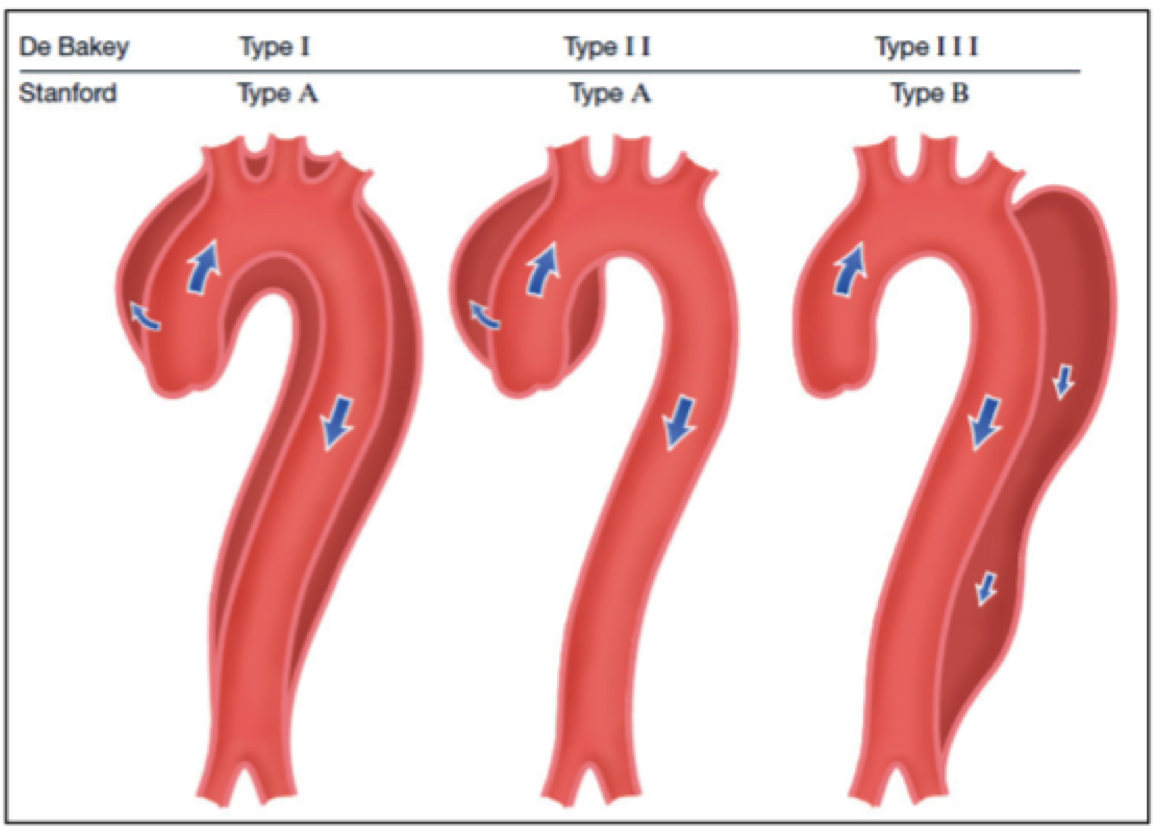
1/ Dreaded DISSECTION!
DeBakey and Stanford class⬇️
RFs: HTN, Male, age
Presents: Abrupt severe pain (chest or back)! Check both💪 BP
Dx: CTA>TEE>TTE
Complications: Propagation 2 RCC/RCA MI (think b4 going to cath lab!) pericardial eff (but try to avoid pericardiocentesis!)
DeBakey and Stanford class⬇️
RFs: HTN, Male, age
Presents: Abrupt severe pain (chest or back)! Check both💪 BP
Dx: CTA>TEE>TTE
Complications: Propagation 2 RCC/RCA MI (think b4 going to cath lab!) pericardial eff (but try to avoid pericardiocentesis!)

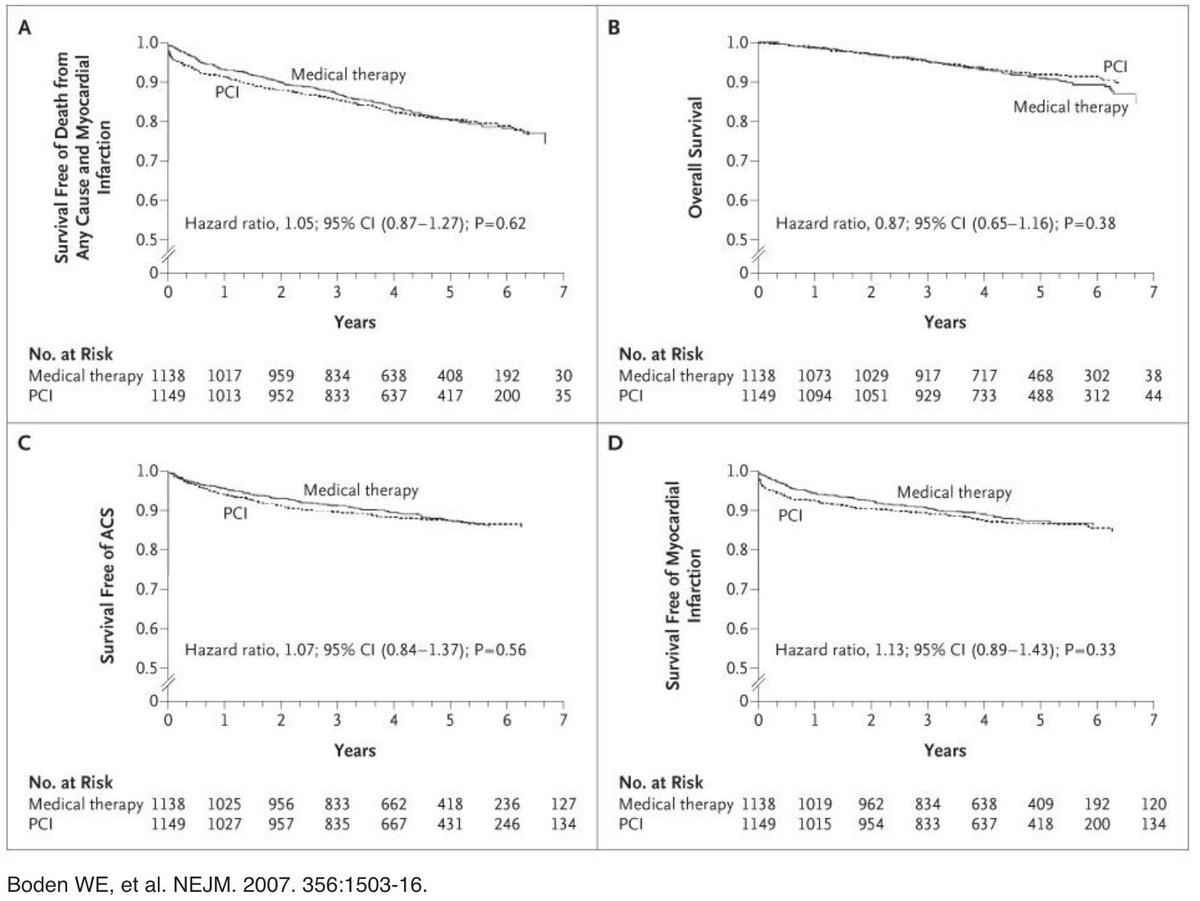
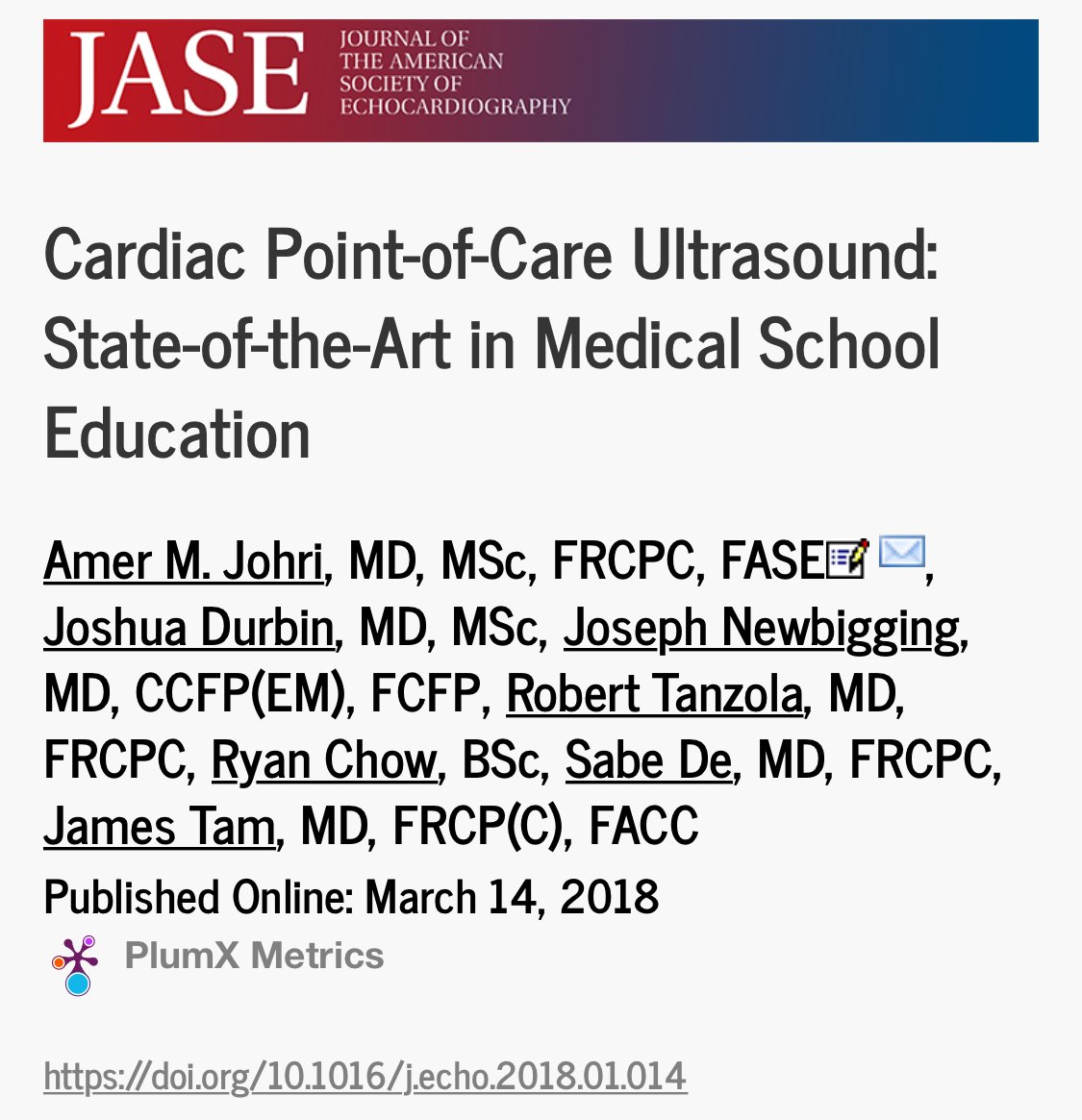
1/10 “To PCI, or Not to PCI, That is the Question” Will Shakespeare, MD
#FITSurvivalGuide
*Per many contentious #cardiotwitter discussions I realize this is loaded topic but I’m going to attempt an early stage #ACCFIT overview while recognizing there is a lot of nuance.
#FITSurvivalGuide
*Per many contentious #cardiotwitter discussions I realize this is loaded topic but I’m going to attempt an early stage #ACCFIT overview while recognizing there is a lot of nuance.

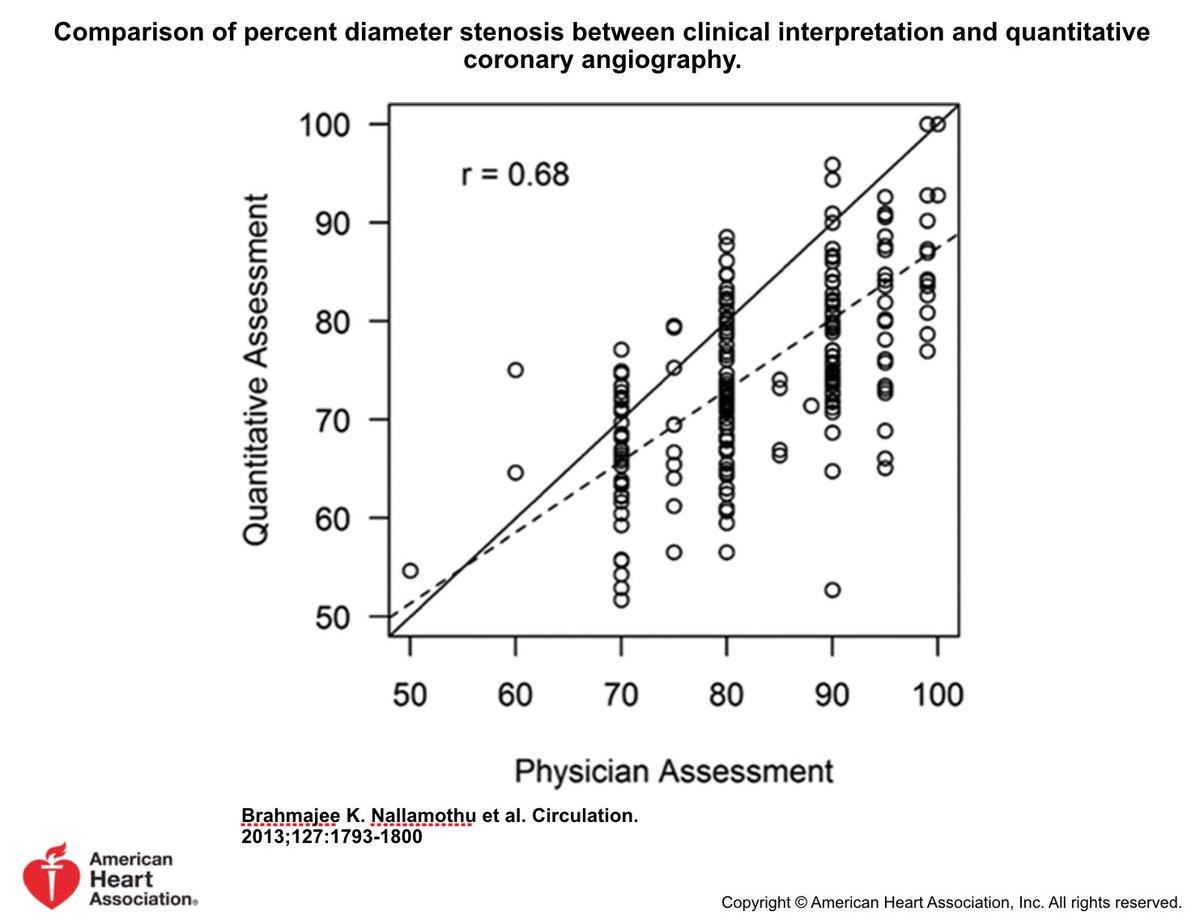
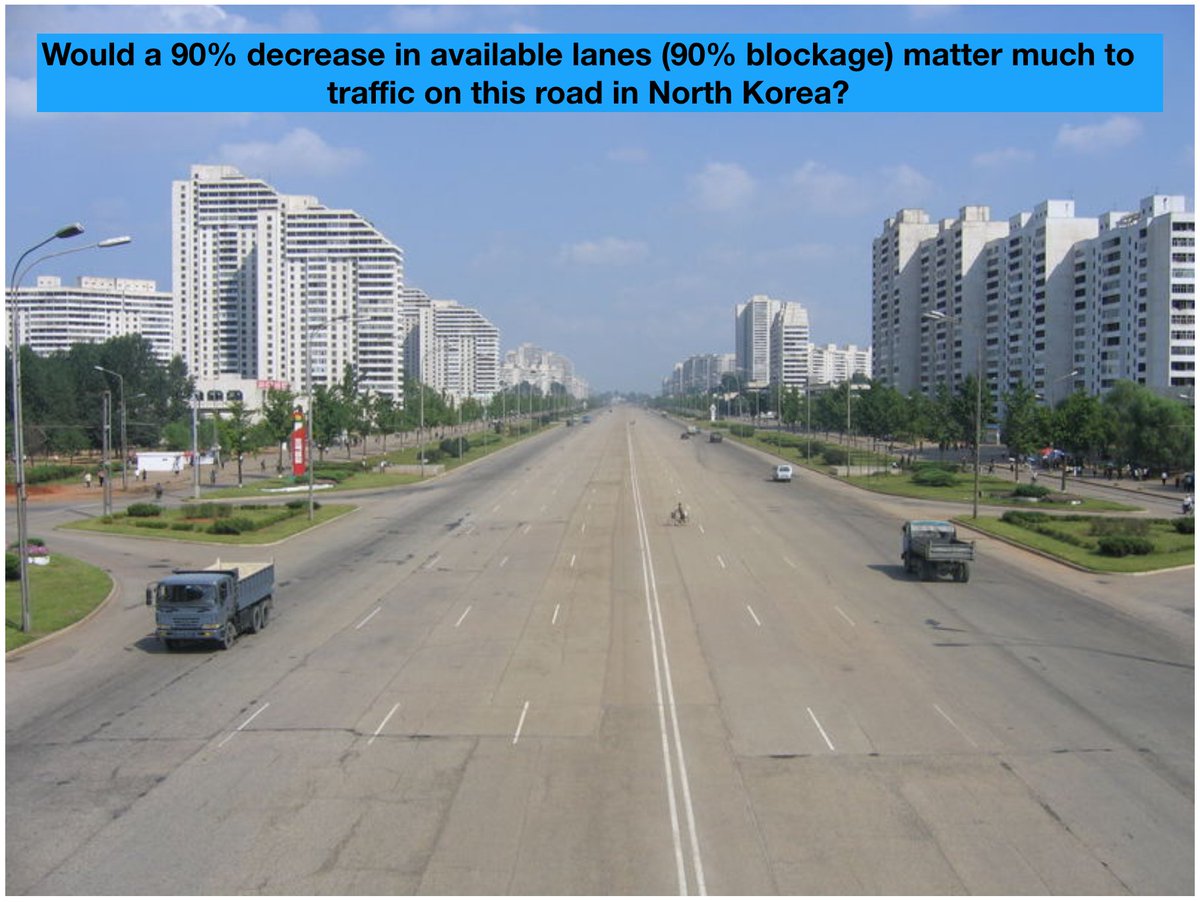
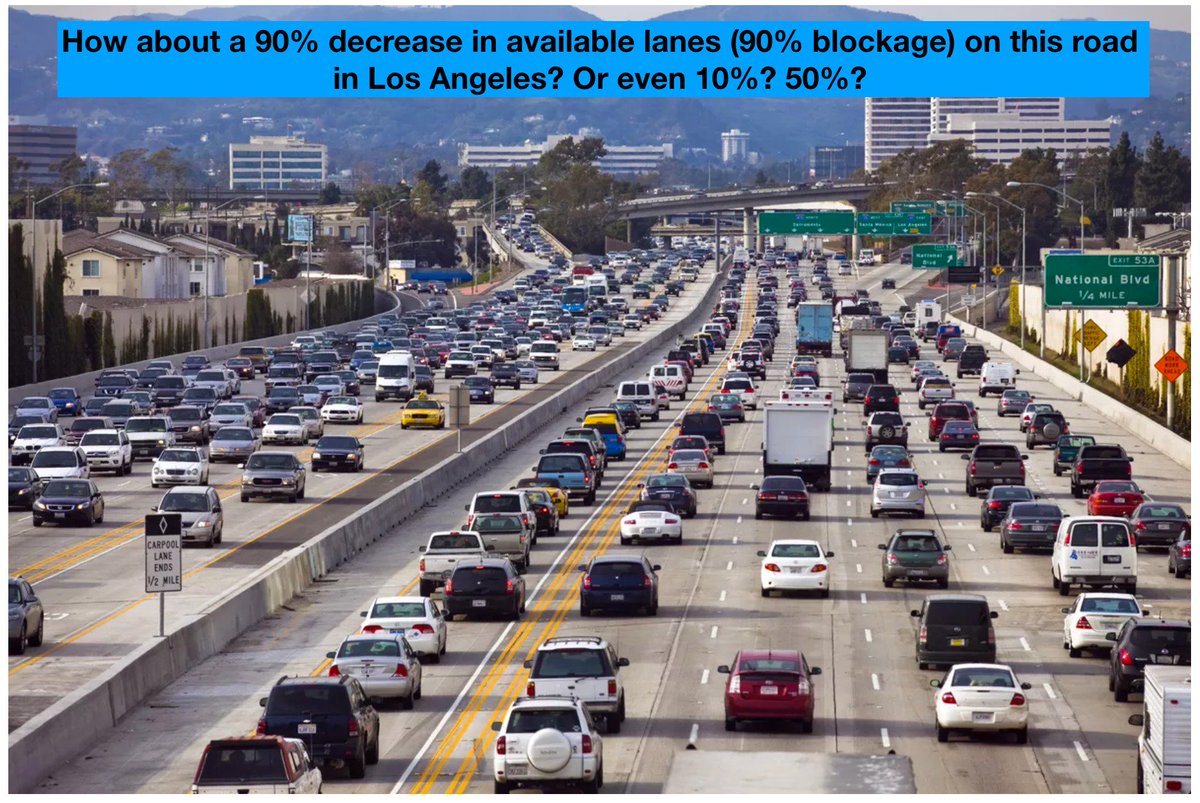
2/10 Why not “See lesion Fix lesion”?
Poor correlation between est'd visual stenosis & quantitative stenosis. And, without noninvasive ischemic data, coronary angio has limited accuracy w/ regard to identifying significance of many stenoses
*STEMI PCI already done @KhandelwalMD
Poor correlation between est'd visual stenosis & quantitative stenosis. And, without noninvasive ischemic data, coronary angio has limited accuracy w/ regard to identifying significance of many stenoses
*STEMI PCI already done @KhandelwalMD
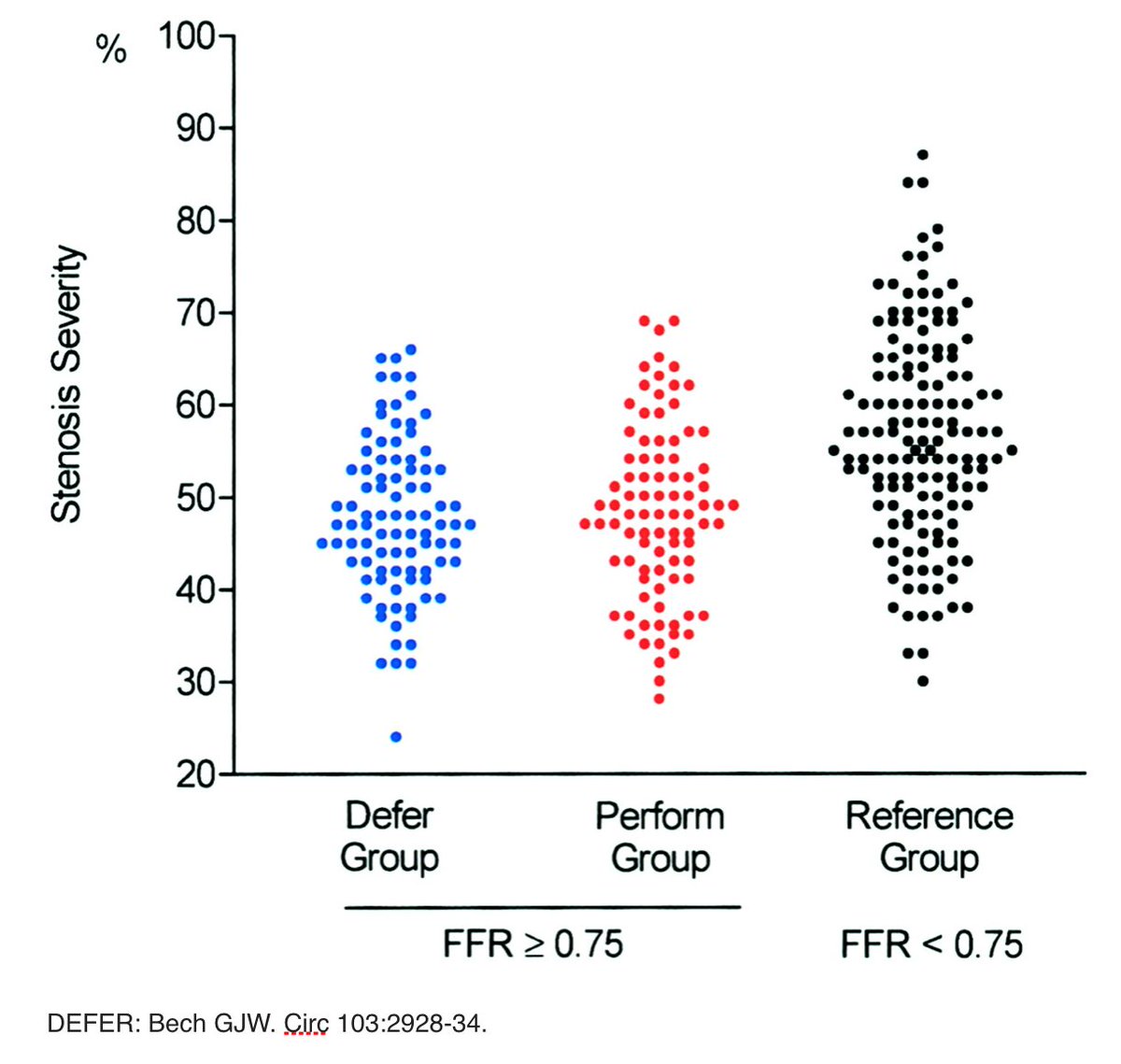
3/10 COURAGE trial (OMT vs OMT and PCI of visually-estimated significant stenoses): No difference death/MI between OMT & OMT/PCI. PCI demonstrated clinical benefit only when treating relevant myocardial ischemia determined by noninvasive testing.